სტივენს-ჯონსონის სინდრომი/ტოქსიკური ეპიდერმული ნეკროლიზი, ფიზიოლოგიური ეფექტების თვალსაზრისით, მსგავსია მეორე ხარისხის დამწვრობისა.
მკურნალობა მოითხოვს მულტიდისციპლინური გუნდის ჩართულობას, რათა პაციენტებმა მიიღონ ჭრილობის ყოველდღიური ოპტიმალური მართვა, კვება, კრიტიკული მკურნალობა, ტკივილის მართვა და დამხმარე ტიპის მოვლა.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
სტივენს-ჯონსონის სინდრომის/ტოქსიკური ეპიდერმული ნეკროლიზის დიაგნოზის შემთხვევაში, რეკომენდებულია პაციენტის გადაყვანა დამწვრობის ცენტრში, ჭრილობების მოვლის სპეციალიზებულ ცენტრში ან დერმატოლოგიური ინტენსიური თერაპიის განყოფილებაში.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ზუსტი მკურნალობა დამოკიდებულია კანის ჩართულობის ხარისხზე, ხოლო როგორც სტივენს-ჯონსონის სინდრომის, ასევე ტოქსიკური ეპიდერმული ნეკროლიზი მიმართ იგივე ზოგადი პრინციპები გამოიყენება. მკურნალობა უნდა დაიწყოს ინდივიდუალურად, კონკრეტული კლინიკური სურათის მიხედვით.[75]Zimmermann S, Sekula P, Venhoff M, et al. Systemic immunomodulating therapies for Stevens-Johnson syndrome and toxic epidermal necrolysis: a systematic review and meta-analysis. JAMA Dermatol. 2017 Jun 1;153(6):514-22.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5817620
http://www.ncbi.nlm.nih.gov/pubmed/28329382?tool=bestpractice.com
[76]Schneider JA, Cohen PR. Stevens-Johnson syndrome and toxic epidermal necrolysis: a concise review with a comprehensive summary of therapeutic interventions emphasizing supportive measures. Adv Ther. 2017 Jun;34(6):1235-44.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5487863
http://www.ncbi.nlm.nih.gov/pubmed/28439852?tool=bestpractice.com
ორივე დაავადებას აქვს ტენდენცია პროგრესირებისკენ რამდენიმე დღის განმავლობაში, ამიტომ საჭიროა ყველა პაციენტის მკაცრი მონიტორინგი.
გადაუდებელი სამედიცინო დახმარება
დიაგნოზის დასმისას გამომწვევი აგენტი უნდა გამოვლინდეს და დაუყოვნებლივ მოცილდეს. ჩვეულებრივ, ეს აღმოჩნდება ახალი წამალი, რომლის მიღება იწყება გამონაყარის დაწყებამდე 2-3 კვირით ადრე.
სტივენს-ჯონსონის სინდრომის/ტოქსიკური ეპიდერმული ნეკროლიზის დროს ყველაზე ხშირად დანიშნული მედიკამენტბი ჩამოთვლილია ეტიოლოგიის ნაწილში. იხილეთ ეტიოლოგია.
სტივენს-ჯონსონის სინდრომის/ტოქსიკური ეპიდერმული ნეკროლიზის მქონე პაციენტები უნდა შეფასდნენ ისევე, როგორც დამწვრობის მქონე პაციენტები. საჭიროა სასუნთქი გზების, სუნთქვის და სისხლის მიმოქცევის შეფასება. იხ კანის დამწვრობა (დიაგნოსტიკური მიდგომა).
არტერიული სისხლის აირები და ჟანგბადით გაჯერება დაგვეხმარება პაციენტის კლინიკური რესპირატორული სტატუსის განსაზღვრაში.
აუცილებელია მთლიანი სხეულის ზედაპირის ფართობის (TBSA) დაზიანების შემოწმება, დაავადების სიმძიმის შესაფასებლად. შეიძლება გამოიყენოთ სხვადასხვა მეთოდები, როგორიცაა უოლასის 9-ების წესი, პალმერი, ლუნდ-ბროუდერის დამწვრობის შეფასების სქემა ან SCORTEN.[55]Lund CC, Browder NC. The estimation of areas of burns. Surg Gynecol Obst. 1944;79:352-8.[57]Wachtel TL, Berry CC, Wachtel EE, et al. The inter-rater reliability of estimating the size of burns from various burn area chart drawings. Burns. 2000 Mar;26(2):156-70.
http://www.ncbi.nlm.nih.gov/pubmed/10716359?tool=bestpractice.com
Wallace rule of 9s
Opens in new window იხილეთ დიაგნოსტიკური მიდგომა.
[Figure caption and citation for the preceding image starts]: "ცხრათა წესი"From Dr Sheridan's personal collection [Citation ends].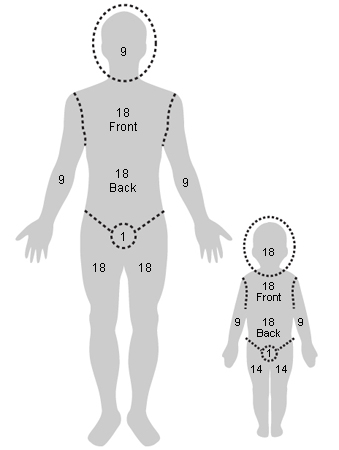 [Figure caption and citation for the preceding image starts]: ლუნდ-ბრაუდერის დიაგრამაFrom Dr Sheridan's personal collection [Citation ends].
[Figure caption and citation for the preceding image starts]: ლუნდ-ბრაუდერის დიაგრამაFrom Dr Sheridan's personal collection [Citation ends].
რაც უფრო მეტია სხეულის ზედაპირის საერთო ფართობის პროცენტული მაჩვენებელი, მით უფრო მეტია სითხეზე მოთხოვნა.[56]Hettiaratchy S, Papini R. Initial management of a major burn: II - assessment and resuscitation. BMJ. 2004 Jul 10;329(7457):101-3.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC449823
http://www.ncbi.nlm.nih.gov/pubmed/15242917?tool=bestpractice.com
განიხილეთ ინტუბაცია და ადრეული ტრაქეოსტომია პაციენტებში, რომელთაც აქვთ პირის ღრუს ჩართულბოა და ჩამოთვლილთაგან ერთ-ერთი:[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
სხეულის საწყისი ზედაპირული ფართობის 70%-ით ან მეტით დაზიანება
დაზიანებული სხეულის ზედაპირული ფართობის პროგრესირება ჰოსპიტალიზაციის I დღიდან III დღემდე >15%-ით
ფონური ნევროლოგიური დიაგნოზი ხელს უშლის სასუნთქი გზების დაცვას
სასუნთქი გზების დაზიანება, რომელიც დადგენილია პირდაპირი ლარინგოსკოპიით.
მტკიცებულებების მიხედვით, ინტუბირებული პაციენტებისთვის სიკვდილობის მაჩვენებელი იზრდება 50%-მდე.[54]de Prost N, Mekontso-Dessap A, Valeyrie-Allanore L, et al. Acute respiratory failure in patients with toxic epidermal necrolysis: clinical features and factors associated with mechanical ventilation. Crit Care Med. 2014 Jan;42(1):118-28.
http://www.ncbi.nlm.nih.gov/pubmed/23989174?tool=bestpractice.com
იმ შემთხვევაში, თუ პაციენტი არ იღებს თერაპიულად ანტიკოაგულანტს, მაგრამ შეზღუდული აქვს გადაადგილების უნარი, პროფილაქტიკურად უნდა დაინიშნოს დაბალმოლეკულური ჰეპარინი.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
მექანიკური თრომბოპროფილაქტიკა გრადუირებული კომპრესიული წინდებით ან წყვეტილი პნევმატური კომპრესიით რეკომენდებულია იმ პაციენტებისთვის, რომლებიც მწვავედ მიმდინარე დაავადების გამო იმყოფებიან თრომბოზის გაზრდილი რისკის ქვეშ და აქვთ სისხლდენა ან მომატებული აქვთ დიდი სისხლდენის ალბათობა.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
სისხლდენის მაღალი რისკის პაციენტებს და მათ, ვისთვისაც ენტერალური კვება შეუძლებელია, უნდა მიეცეთ პროტონის ტუმბოს ინჰიბიტორი სტრესინდუცირებული გასტრიტისა და ნაწლავის წყლულის თავიდან ასაცილებლად.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
სტივენს-ჯონსონის სინდრომის/ტოქსიკური ეპიდერმული ნეკროლიზის შემთხვევაში ყველა პაციენტის საწყისი შეფასების ნაწილია პოტენციური ორალური, თვალის და უროგენიტალური ჩართულობის შეფასება.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ჭრილობის მოვლა
ჭრილობის მოვლა შესაძლებელია კონსერვატიულად ან ქირურგიულად. ეს დამოკიდებულია ინდივიდუალურ შემთხვევებზე.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
კონსერვატიული მოვლის რეკომენდაციებია:[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
მოწყვეტილი ეპიდერმისის, როგორც ბიოლოგიური სახვევის შენარჩუნება
ნახვევების შეცვლის სიხშირის შეზღუდვა
ჰაერ-სითხოვანი საწოლების გამოყენება
არაწებოვანი სახვევების გამოყენება
ჭრილობების ლიზისის და დრენაჟის გამოყენება მხოლოდ პაციენტის კომფორტისთვის
სახვევის შეცვლისას ჭრილობების გაწმენდა სტერილური წყლით, ნორმალური ფიზიოლოგიური ხსნარით ან განზავებული ქლორჰექსიდინით.
დამარბილებლების გამოყენება მთელ ეპიდერმისზე კანის ბარიერული ფუნქციის გასაძლიერებლად, სითხის დაკარგვის შესამცირებლად და ხელახალი ეპითელიზაციის ხელშესაწყობად.
ანტიბაქტერიული თვისებების გამო არაწებოვანი, ვერცხლით გაჟღენთილი პირველადი სახვევების გამოყენების გათვალისწინება, სახვევის შეცვლის საჭიროების შემცირება და პაციენტის კომფორტის გაუმჯობესება
მეორადი შთანმთქმელი სახვევების გამოყენება ექსუდატის გასაკონტროლებლად.
სტივენს-ჯონსონის სინდრომის/ტოქსიკური ეპიდერმული ნეკროლიზის შემთხვევში ჭრილობის მოვლის ქირურგიული მიდგომა მიჰყვება დამწვრობის მართვის პრაქტიკას: როგორც კი მოწყვეტილი ეპიდერმისი ქირურგიულალ მოცილდება, ჭრილობები იფარება ბიოლოგიური საფენით, როგორიცაა ქსენოტრანსპლანტატი (ღორის კანი), ალოტრანსპლანტატი (სხეულის კანი) ან სინთეტიკური სახვევი.[77]Nizamoglu M, Ward JA, Frew Q, et al. Improving mortality outcomes of Stevens Johnson syndrome/toxic epidermal necrolysis: a regional burns centre experience. Burns. 2018 May;44(3):603-11.
http://www.ncbi.nlm.nih.gov/pubmed/29029855?tool=bestpractice.com
შეხორცებისას, განიხილეთ არაწებოვანი ვერცხლით გაჟღენთილი სახვევის გამოყენება, სახვევის შეცვლის დროს და პაციენტის კომფორტის გაუმჯობესების მიზნით.
დიდი ბრიტანეთის გაიდლაინების რეკომენდაციით, პაციენტები გადაყვანილ უნდა იყვნენ დამწვრობის განყოფილებაში ქირურგიული წესით გასუფთავებისა და ჭრილობის მოვლისთვის, თუ ვლინდება ტოქსიკური ეპიდერმული ნეკროლიზი (>30% სხეულის სრული ზედაპირის ეპიდერმული დაკარგვა) და შემდეგი მტკიცებულებები:[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
მას შემდეგ, რაც რეგენერირდება კანი(დაახლოებით 2-დან 3 კვირამდე ვადაში), შესაძლოა სარგებლიანი იყოს დამარბილბელი საშუალებები, ელასტიკურობის შენარჩუნებისა და გამოშრობის საპრევენციოდ.
სითხის მართვა
თუკი ვლინდება ხშირი პირღებინება, შეიძლება განვითარდეს გაუწყლოება. გარდა ამისა, კანის აქერცვლის ხარისხის მიხედვით პაციენტმა შეიძლება დაკარგოს სითხის მნიშვნელოვანი რაოდენობა კანის დამწვარი ზედაპირიდან. ყოველდღიურად უნდა მიმდინარეობდეს ელექტროლიტებისა და სითხის ბალანსის მონიტორინგი.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
თუ პაციენტს შეუძლია სითხეების პერორულად მიღება, უნდა წავახალისოთ ისინი, რომ მიიღონ სითხე. სხვა შემთხვევაში საჭიროა ინტრავენური გადასხმები, როგორიცაა რინგერის ლაქტატის ხსნარი ან 0.9% ნატრიუმის ქლორიდი, პაციენტის ჰიდრატაციის მიზნით. შემთხვევათა სერიის ერთ-ერთი კვლევით დგინდება, რომ დაახლოებით 2 მლ/კგ/% სხეულის ზედაპირის საერთო ფართობი შეიძლება იყოს ადეკვატური, თუკი არ არსებობს სხვა გართულებები.[78]Shiga S, Cartotto R. What are the fluid requirements in toxic epidermal necrolysis? J Burn Care Res. 2010 Jan-Feb;31(1):100-4.
http://www.ncbi.nlm.nih.gov/pubmed/20061843?tool=bestpractice.com
მიუხედავად საჭირო სითხის გამოთვლილი რაოდენობისა, პაციენტის რეაქციის კლინიკური სურათი მეტისმეტად მნიშვნელოვანია. რეჰიდრატაციის მონიტორინგი ხორციელდება შარდის გამოყოფაზე დაკვირვებით. მნიშვნელოვანია, რომ ზრდასრულის მიერ შარდის გამოყოფა შეადგენდეს 0.5 მლ/კგ/სთ-ს (30-დან 50 მლ / საათში), ხოლო <30 კგ წონის ბავშვებში - 1 მლ/კგ/სთ-ს.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
რეჰიდრატაციის გაძლიერება ან შესუსტება შარდის გამოყოფაზეა დამოკიდებული.
ტკივილის მართვა
ანალგეზია უნდა ჩატარდეს სიმპტომების სიმძიმის მიხედვით, რათა უზრუნველყოფილი იყოს კომფორტი დასვენების დროს. ტკივილის დონე უნდა შეფასდეს ყოველ 4 საათში ერთხელ და ვალიდური ტკივილის შემფასებელი ინსტრუმენტის გამოყენებით სულ მცირე დღეში ერთხერ.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
სახვევების შეცვლის დროს საჭიროეა უფრო მეტი ტკივილგამაყუჩებლებს.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
თუ მსუბუქი ტკივილი არ იხსნება პარაცეტამოლით, უნდა განიხილებოდეს პერორული ოპიოიდი, როგორიცაა ტრამადოლი.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
მორფინი ან ფენტანილი შეიძლება საჭირო გახდეს ზომიერი ან ძლიერი ტკივილის შემთხვევაში. დაბალი დოზით კეტამინი შეიძლება ჩაითვალოს სტივენს-ჯონსონის სინდრომით/ტოქსიკური ეპიდერმული ნეკროლიზით გამოწვეული ტკივილის ალტერნატიულ ან დამხმარე თერაპიად.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
გაბაპენტინი და პრეგაბალინი ორივე მოქმედებს ნეიროპათიურ ტკივილზე და შეიძლება შეამციროს ოპიოიდების მოხმარება როგორც მწვავე, ასევე შეხორცების ფაზაში სტივენს-ჯონსონის სინდრომის მქონე პაციენტებისთვის.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
თირკმელების ან კუჭის დაზიანების რისკის გაზრდის გამო თავიდან უნდა აირიდოთ არასტეროიდული ანთების საწინააღმდეგო საშუალებები.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ინტრავენური იმუნოგლობულინი და ციკლოსპორინი
არ არსებობს მკაფიო მითითებები ინტრავენური იმუნოგლობულინის (IVIg) გამოყენებასთან დაკავშირებით. ზოგიერთი კლინიცისტი იყენებს IVIG-ს სწრაფად პროგრესირებადი გამონაყარის დროს, რომელიც მოიცავს სხეულის ზედაპირის საერთო ფართობის მინიმუმ 6%-ს. სხვები ნიშნავენ ინტრავენურ იმუნოგლობულინს მხოლოდ მაშინ, როდესაც დაზიანებულია სხეულის ზედაპირის საერთო ფართობის (TBSA) 20%. არ არსებობს მკურნალობის ავტორიტეტული რანდომიზებული კონტროლირებადი კვლევა. არსებული ლიტერატურა შედგება მცირე რეტროსპექტიული და პროსპექტიული სერიებისგან. ამ მცირე კლინიკური კვლევების მიმოხილვით ვლინდება IVIg -ის გამოყენების რამდენიმე დადებითი ეფექტი და არანაირი მნიშვნელოვანი გართულება.[2]Dodiuk-Gad RP, Chung WH, Valeyrie-Allanore L, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: an update. Am J Clin Dermatol. 2015 Dec;16(6):475-93.
http://www.ncbi.nlm.nih.gov/pubmed/26481651?tool=bestpractice.com
[24]Mockenhaupt M. Stevens-Johnson syndrome and toxic epidermal necrolysis: clinical patterns, diagnostic considerations, etiology, and therapeutic management. Semin Cutan Med Surg. 2014 Mar;33(1):10-6.
http://www.ncbi.nlm.nih.gov/pubmed/25037254?tool=bestpractice.com
[42]Schwartz RA, McDonough PH, Lee BW. Toxic epidermal necrolysis. Part I: introduction, history, classification, clinical features, systemic manifestations, etiology, and immunopathogenesis. J Am Acad Dermatol. 2013 Aug;69(2):173.
http://www.ncbi.nlm.nih.gov/pubmed/23866878?tool=bestpractice.com
[44]Schwartz RA, McDonough PH, Lee BW. Toxic epidermal necrolysis. Part II: prognosis, sequelae, diagnosis, differential diagnosis, prevention, and treatment. J Am Acad Dermatol. 2013 Aug;69(2):187.
http://www.ncbi.nlm.nih.gov/pubmed/23866879?tool=bestpractice.com
[79]Barron SJ, Del Vecchio MT, Aronoff SC. Intravenous immunoglobulin in the treatment of Stevens-Johnson syndrome and toxic epidermal necrolysis: a meta-analysis with meta-regression of observational studies. Int J Dermatol. 2015 Jan;54(1):108-15.
http://www.ncbi.nlm.nih.gov/pubmed/24697283?tool=bestpractice.com
[80]Aires DJ, Fraga G, Korentager R, et al. Early treatment with nonsucrose intravenous immunoglobulin in a burn unit reduces toxic epidermal necrolysis mortality. J Drugs Dermatol. 2013 Jun 1;12(6):679-84.
http://www.ncbi.nlm.nih.gov/pubmed/23839186?tool=bestpractice.com
[81]Enk A, Hadaschik E, Eming R, et al. European guidelines (S1) on the use of high-dose intravenous immunoglobulin in dermatology. J Dtsch Dermatol Ges. 2017 Feb;15(2):228-41.
http://www.ncbi.nlm.nih.gov/pubmed/28036140?tool=bestpractice.com
სტივენს-ჯონსონის სინდრომის/ტოქსიკური ეპიდერმული ნეკროლიზის თანხვედრის შემთხვევაში, მრავალ დამწვრობის ცენტრში იყებნეენ ინტრავენურ იმუნოგლობულინს, სწრაფად პროგრესირებადი გამონაყარის შემთხვვაში და როდესაც პაციენტი კლინიკურად მიიჩნევა შესაფესირისად.
არსებობს TEN-ის ციკლოსპორინით წარმატებული მკურნალობის სპორადული შემთხვევები. SJS / TEN -ის მქონე 71 პაციენტის სამედიცინო ბარათების რეტროსპექტულ ანალიზში, ციკლოსპორინი დაკავშირებული იყო სიკვდილის მოსალოდნელზე ნაკლებ შემთხვევებთან (სიკვდილობის სტანდარტიზებული მაჩვენებელია 0,43), მაშინ როდესაც ინტრავენური იმუნოგლობულინი დაკავშირებული იყო სიკვდილობის მატებასთან (სიკვდილობის სტანდარტიზებული მაჩვენებელია 1,43).[82]Kirchhof MG, Miliszewski MA, Sikora S, et al. Retrospective review of Stevens-Johnson syndrome/toxic epidermal necrolysis treatment comparing intravenous immunoglobulin with cyclosporine. J Am Acad Dermatol. 2014 Nov;71(5):941-7.
http://www.ncbi.nlm.nih.gov/pubmed/25087214?tool=bestpractice.com
სხვა კვლევით, რომელიც ტარდებოდა იმ 16 პაციენტზე, რომლებიც იღებდნენ ციკლოსპორინს, გამოვლინდა სიკვდილობის უფრო დაბალი მაჩვენებელი, ვიდრე პროგნოზირებული იყო SCORTEN ქულით.[83]Balai M, Meena M, Mittal A, et al. Cyclosporine in Stevens-Johnson syndrome and toxic epidermal necrolysis: experience from a tertiary care centre of South Rajasthan. Indian Dermatol Online J. 2021 Jan-Feb;12(1):116-22.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7982025
http://www.ncbi.nlm.nih.gov/pubmed/33768032?tool=bestpractice.com
ერთი მცირე (n=29), ღია ეტიკეტის, II ფაზის კვლევის შედეგებით ვლინდება, რომ ციკლოსპორინმა შეიძლება შეამციროს სიკვდილობა და ეპიდერმული აქერცვლის პროგრესირება სტივენს-ჯონსონის სინდრომის/ტოქსიკური ეპიდერმული ნეკროლიზის შემთხვევებში. საშუალოდ 77%-იანი სხეულის სრული ზედაპირული ფართობის დაზიანების მქონე 12 პაციენტზე ჩატარებულ მცირე კვლევაში, რომლებიც მკურნალობდნენ ციკლოსპორინით და პლაზმაფერეზით, დაფიქსირდა სიკვდილის ერთი შემთხვევა.[84]Valeyrie-Allanore L, Wolkenstein P, Brochard L, et al. Open trial of ciclosporin treatment for Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 2010 Oct;163(4):847-53.
http://www.ncbi.nlm.nih.gov/pubmed/20500799?tool=bestpractice.com
სხვა მეტა-ანალიზით დადგინდა, რომ ციკლოსპორინის გამოყენება ეპიდერმული ნეკროლიზის დროს ეფექტურად ამცირებს სიკვდილის რისკს.[75]Zimmermann S, Sekula P, Venhoff M, et al. Systemic immunomodulating therapies for Stevens-Johnson syndrome and toxic epidermal necrolysis: a systematic review and meta-analysis. JAMA Dermatol. 2017 Jun 1;153(6):514-22.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5817620
http://www.ncbi.nlm.nih.gov/pubmed/28329382?tool=bestpractice.com
[85]Ng QX, De Deyn MLZQ, Venkatanarayanan N, et al. A meta-analysis of cyclosporine treatment for Stevens-Johnson syndrome/toxic epidermal necrolysis. J Inflamm Res. 2018 Mar 28;11:135-42.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5880515
http://www.ncbi.nlm.nih.gov/pubmed/29636627?tool=bestpractice.com
[86]González-Herrada C, Rodríguez-Martín S, Cachafeiro L, et al. Cyclosporine use in epidermal necrolysis is associated with an important mortality reduction: evidence from three different approaches. J Invest Dermatol. 2017 Oct;137(10):2092-100.
https://www.jidonline.org/article/S0022-202X(17)31645-7/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/28634032?tool=bestpractice.com
[87]Roujeau JC, Mockenhaupt M, Guillaume JC, et al. New evidence supporting cyclosporine efficacy in epidermal necrolysis. J Invest Dermatol. 2017 Oct;137(10):2047-9.
https://www.jidonline.org/article/S0022-202X(17)32758-6/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/28941473?tool=bestpractice.com
პირის ღრუს ჩართულობა
პირის ღრუს ჩართვა გვხვდება სტივენს-ჯონსონის სინდრომის/ტოქსიკური ეპიდერმული ნეკროლიზის შემთხვევათა უმრავლესობაში, რაც იწვევს ტკივილს, პერორული მიღების დარღვევას და პირის ღრუს არასასურველ ჰიგიენას. პაციენტებთან უნდა გამოვიკვლიოთ პირის ღრუ დაავადების გამოვლინებისას ყოველდღიურად მწვავე მიმდინარეობის ფაზაში.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
მწვავე ავადმყოფობის განმავლობაში რეკომენდებულია ტუჩებზე ვაზელინის მალამოს წასმა ყოველ 2 საათში.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ტკივილის მართვა
ტკივილის ხანმოკლე შემსუბუქების მიზნით, საჭიროა პირის ღრუს ამორეცხვა ან სპრეის გამოყენება ადგილობრივი საანესთეზიო, ანთების საწინააღმდეგო და ტკივილგამაყუჩებელი საშუალებებით(მაგ. ბლანტი ლიდოკაინი, ბენზიდამინი), განსაკუთრებით ჭამამდე ან პირის ღრუს გაწმენდის წინ.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ადგილობრივი პერორული გარსიანი აგენტები რეკომენდებულია ტკივილის შესამცირებლად პაციენტებში, რომელთაც აღენიშნებათ პირის ღრუს ლორწოვანის ჩართულობა.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
პირის ღრუს ჰიგიენა
პაციენტის პირი ყოველდღიურად უნდა გასუფთავდეს თბილი მარილიანი სავლებით ან სპეციალური ღრუბლით.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ლორწოვანი გარსის ბაქტერიული კოლონიზაციის შესამცირებლად უნდა გამოიყენოთ პირის ღრუს ანტისეპტიკური სავლებები (მაგ., განზავებული ქლორჰექსიდინი).[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
დაავადების მწვავე ფაზაში რეკომენდებულია ძლიერი ადგილობრივი კორტიკოსტეროიდული პირის ღრუს ამოსარეცხი (მაგ., დექსამეტაზონი) ან ულტრაძლიერი ადგილობრივი კორტიკოსტეროიდული მალამო.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
კვება
თუ შესაძლებელია, კვება უნდა წარმოევდეს პერორულად. თუ ეს შეუძლებელია, უნდა უზრუნველჰყოთ ენტერული კვება ნაზოგასტრული მილით.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ნაზოგასტრული მილის ჩადგმა დაუშვებელია პაციენტებში, რომელთაც დაზიანებული აქვთ ნაზოფარინგული ლორწოვანი გარსი.
კვებითი მხარდაჭერა უნდა მოიცავდეს 30-35 კკალ/კგ-ს, მკაცრი გლიკემიური კონტრლის ფონზე.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
თუ ადეკვატური კალორაჟის მიღება ვერ ხერხდება ენტერული კვებით, უნდა დაემატოს პარენტერული გზაც.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
თვალის დაზიანება
ყველა იმ პაციენტთან, რომელთანაც ვლინდება სტივენს-ჯონსონის სინდრომის/ტოქსიკური ეპიდერმული ნეკროლიზის ნიშნები და სიმპტომები, უნდა ჩატარდეს ოფთალმოლოგის კონსულტაცია და სრული გამოკვლევა ჰოსპიტალიზაციის მომენტში, ასევე ყოველდღიურად დაავადების მწვავე ფაზაში, სანამ არ დადასტურდება, რომ არ არის მხედველობის გაუარესება.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
[88]Gregory DG. New grading system and treatment guidelines for the acute ocular manifestations of Stevens-Johnson syndrome. Ophthalmology. 2016 Aug;123(8):1653-8.
http://www.ncbi.nlm.nih.gov/pubmed/27297404?tool=bestpractice.com
შემდგომი დაკვირვების ფორმა უნდა განისაზღვროს თითოეულ შემთხვევაში ინდივიდუალურად.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
თვალის დაზიანების შემთხვევაში, ლუბრიკანტები (წვეთები და მალამოები) უნდა დაინიშნოს ყოველ 2 საათში ერთხელ ავადმყოფობის მწვავე სტადიაზე.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
რეკომენდებულია თვალის მთლიანი ზედაპირის ყოველდღიური გამოკვლევა (ქუთუთოების კანი, ქუთუთოს კიდე, კონიუნქტივა და რქოვანა).[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ეს უნდა მოიცავდეს ქუთუთოს თაღის და ხრტილის კონიუნქტივას ეპითელიუმის დეფექტების და ადრეული სიმბლეფარის შეფასებას ქუთუთოების ამობრუნების გზით, როდესაც თვალიც გადატრიალებულია.
რქოვანას დაზიანებების, ან თვალში უცხო სხულების ან ნაწილაკების და ცრემლის წარმოქმნის დარღვევის გამოსავლენად თითოეულ პაციენტს უნდა ჩაუტარდეს გრამის წესით შეღებვის პროცედურა.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ქუთუთოების მოსვენებული მდგომარეობა უნდა შეფასდეს ლაგოფთალმზე, განსაკუთრებით უგონო პაციენტებში, რადგან აუცილებელია რქოვანზე ექსპოზიციის პრევენცია.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ამნიოტური მემბრანის ტრანსპლანტაცია უნდა განიხილებოდეს ნებისმიერი პაციენტის თავდაპირველი შეფასებისას, რომელზეც არსებობს ეჭვი, რომ აქვს სტივენს-ჯონსონის სინდრომი/ტოქსიკური ეპიდერმული ნეკროლიზი და ასევე ყოველი შემდგომი გამოკვლევის დროს მწვავე ფაზაში.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
თვალის მთელი ზედაპირის დაფარვა ამნიოტური მემბრანით, ინტენსიური მოკლევადიანი კორტიკოსტეროიდებით მკურნალობასთან ერთად, სტივენს-ჯონსონის სინდრომის და ტოქსიკური ეპიდერმული ნეკროლიზის მწვავე ფაზაში, დაკავშირებულია მხედველობის შენარჩუნებასთან და თვალის დაუზიანებელ ზედაპირთან.[88]Gregory DG. New grading system and treatment guidelines for the acute ocular manifestations of Stevens-Johnson syndrome. Ophthalmology. 2016 Aug;123(8):1653-8.
http://www.ncbi.nlm.nih.gov/pubmed/27297404?tool=bestpractice.com
შარდ-სასქესო სისტემის დაზიანება
შარდ-სასქესო სისტემის დაზიანება ვითარდება იმ ქალებისა და მამაკაცების დაახლოებით 70%-ში, რომელთაც აღენიშნებათ სტივენს-ჯონსონის სინდრომი/ტოქსიკური ეპიდერმული ნეკროლიზი.[89]Van Batavia JP, Chu DI, Long CJ, et al. Genitourinary involvement and management in children with Stevens-Johnson syndrome and toxic epidermal necrolysis. J Pediatr Urol. 2017 Oct;13(5):490.e1-7.
http://www.ncbi.nlm.nih.gov/pubmed/28314701?tool=bestpractice.com
[90]Meneux E, Wolkenstein P, Haddad B, et al. Vulvovaginal involvement in toxic epidermal necrolysis: a retrospective study of 40 cases. Obstet Gynecol. 1998 Feb;91(2):283-7.
http://www.ncbi.nlm.nih.gov/pubmed/9469290?tool=bestpractice.com
ამან შეიძლება გამოიწვიოს სათესლე პარკის/სასქესო ბაგის, პენისის/ვულვის ეროზია; დიზურია; ჰემატურია; შარდის შეკავება; და გრძელვადიანი შედეგები, როგორიცაა ურეთრის სტენოზი და ნაწიბურები, ქსეროზი, ფიმოზი, დისპარეუნია, ქრონიკული ტკივილი, სისხლდენა, სექსუალური დისფუნქცია, უნაყოფობა და შფოთვა.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
სტივენს-ჯონსონის სინდრომი/ტოქსიკური ეპიდერმული ნეკროლიზის შემთხვევაში, ყველა პაციენტის უროგენიტალური ტრაქტის გამოკვლევა რეკომენდებულია პირველადი შეფასებისას და ყოველდღიურად ჰოსპიტალიზაციის დროს.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
საშარდე კათეტერის ჩადგმა საჭიროა, თუ უროგენიტალური დაზიანება იწვევს მნიშვნელოვან დიზურიას/შეკავებას.[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
ვულვარ/უროგენიტალური კანი/ლორწოვანი გარსი უნდა იყოს დაფარული მალამოთი და/ან მალამოს მარლით, რათა შემცირდეს ტკივილი, შეამციროს ადჰეზიის წარმოქმნა და ხელი შეუწყოს შეხორცებას დაავადების მწვავე ფაზაში.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ქალებისთვის, რომლებზეც არსებობს ვაგინალური დაზიანების ეჭვი, შეიძლება გამოვიყენოთ ინტრავაგინალური დილატორი ან:[63]Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br J Dermatol. 2016 Jun;174(6):1194-227.
https://onlinelibrary.wiley.com/doi/10.1111/bjd.14530
http://www.ncbi.nlm.nih.gov/pubmed/27317286?tool=bestpractice.com
[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
არასტეროიდული მალამო (მაგ., ვაზელინის ჟელე), საჭიროებისამებრ ხელახლა წასმით ბარიერული დაცვის შესანარჩუნებლად და/ან
მძლავრი კორტიკოსტეროიდული მალამო, თუ აღინიშნება აქტიური ანთება.
ადგილობრივი კორტიკოსტეროიდების დოზის კლება უნდა ეფუძნებოდეს კლინიკურ გაუმჯობესების დინამიკას.
თუ საეჭვოა ვაგინალური კანდიდოზი, გამოიყენეთ კალიუმის ჰიდროქსიდის პრეპარატი და სოკოს კულტურა და დაიწყეთ მკურნალობა შესაბამისი ანტიფუნგალური მედიკამენტებით.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
საშოს ლორწოვანი გარსის შეხორცების ხელშეწყობის მიზნით, მედიკამენტების ჩანაცვლება შესაძლებელია ესტროგენის კრემით.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
ინტრავაგინალური დილატორები შეიძლება მოთავსდეს ჩანაცვლებამდე მაქსიმუმ 24 საათით ადრე.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
თუ პაციენტებისთვის ინტრავაგინალური დილატორი დისკომფორტს ქმნის, შესაძლებელია მედიკამენტის გამოყენება ვაგინალური აპლიკატორით.
მენსტრუაციის სუპრესიამ შეიძლება შეამციროს ვაგინალური ადენოზისა და ენდომეტრიოზის რისკი და შეიძლება განვიხილოთ ქალებში, რომლებსაც აქვთ გენიტალური ლორწოვანი გარსის მძიმე დაზიანება.[74]Seminario-Vidal L, Kroshinsky D, Malachowski SJ, et al. Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. 2020 Jun;82(6):1553-67.
http://www.ncbi.nlm.nih.gov/pubmed/32151629?tool=bestpractice.com
შრომის თერაპია და ფიზიოთერაპია
პაციენტებს შეიძლება აღენიშნებოდეთ მოძრაობის შეზღუდვა, კუნთოვანი ძალის დაქვეითებით. პაციენტებმა ყოველდღიურად უნდა ივარჯიშონ თავიანთი შესაძლებლობების ფარგლებში ფიზიოთერაპევტის და საჭიროების შემთხვევაში, შრომითი თერაპევტის თანხლებით.[44]Schwartz RA, McDonough PH, Lee BW. Toxic epidermal necrolysis. Part II: prognosis, sequelae, diagnosis, differential diagnosis, prevention, and treatment. J Am Acad Dermatol. 2013 Aug;69(2):187.
http://www.ncbi.nlm.nih.gov/pubmed/23866879?tool=bestpractice.com