მუცლის აორტის ანევრიზმა
- მიმოხილვა
- თეორია
- დიაგნოზი
- მართვა
- მეთვალყურეობა
- წყაროები
მკურნალობის ალგორითმი
მიაქციეთ ყურადღება, რომ ფორმულა/შეყვანის გზა და დოზა შეიძლება განსხვავებული იყოს მედიკამენტების დასახელების და ბრენდის, ფორმულარის ან გეოგრაფიული ადგილმდებარეობის მიხედვით. მკურნალობის შესახებ რეკომენდაციები სპეციფიკურია პაციენტის ჯგუფების მიხედვით: იხილეთ გაფრთხილება
გამსკდარი მუცლის აორტის ანევრიზმა (AAA)
სტანდარტული რეანიმაციული ღონისძიებები
სტანდარტული რეანიმაციული ღონისძიებები იწყება დაუყოვნებლივ. ესენია: სასუნთქი გზების მართვა (დამატებითი ჟანგბადის ან ენდოტრაქეული ინტუბაცია და დამხმარე ვენტილაცია, თუ პაციენტი უგონო მდგომარეობაშია); ინტრავენური წვდომის უზრუნველყოფა (ცენტრალური ვენური კათეტერი); არტერიული კათეტერი და შარდის კათეტერი; სისხლის პროდუქტების ხელმისაწვდომობის უზრუნველყოფა (შეფუთული წითელი უჯრედები, თრომბოციტები და ახლად გაყინული პლაზმა) და ტრანსფუზია რეანიმაციისთვის, მძიმე ანემიისა და კოაგულოპათიის მიზნით; და საანესთეზიო, ინტენსიური თერაპიის განყოფილების (ICU) და საოპერაციო ჯგუფების შეტყობინება.
სითხის აგრესიულმა ჩანაცვლებითმა თერაპიამ შეიძლება გამოიწვიოს განზავება და ჰიპოთერმული კოაგულოპათია, და მეორადად - თრომბის მოწყვეტა სისხლის ნაკადის ზრდის, პერფუზიის წნევის მომატებისა და სისხლის ვისკოზურობის დაქვეითების გამო, რაც თავის მხრივ იწვევს ხელახალ სისხლდენას.[116]Roberts K, Revell M, Youssef H, et al. Hypotensive resuscitation in patients with ruptured abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. 2006 Apr;31(4):339-44. http://www.ncbi.nlm.nih.gov/pubmed/16388972?tool=bestpractice.com [117]Ohki T, Veith FJ. Endovascular grafts and other image-guided catheter-based adjuncts to improve the treatment of ruptured aortoiliac aneurysms. Ann Surg. 2000 Oct;232(4):466-79. http://www.ncbi.nlm.nih.gov/pubmed/10998645?tool=bestpractice.com ოპერაციამდე რეკომენდებულია სამიზნე სისტოლური წნევა იყოს 50-79 მმ.ვწყ.სვ.-ს ფარგლებში და სითხეების შეზღუდვა.[116]Roberts K, Revell M, Youssef H, et al. Hypotensive resuscitation in patients with ruptured abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. 2006 Apr;31(4):339-44. http://www.ncbi.nlm.nih.gov/pubmed/16388972?tool=bestpractice.com [117]Ohki T, Veith FJ. Endovascular grafts and other image-guided catheter-based adjuncts to improve the treatment of ruptured aortoiliac aneurysms. Ann Surg. 2000 Oct;232(4):466-79. http://www.ncbi.nlm.nih.gov/pubmed/10998645?tool=bestpractice.com ამერიკის კარდიოლოგთა კოლეჯი/ამერიკის გულის ასოციაციის პრაქტიკული გაიდლაინი იყენებს შემდეგ დაყოფას:[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com თუმცა რეკომენდებული მიზნები განსხვავდება და არ არსებობს კონსენსუსი გლობალურ გაიდლაინ ჯგუფებს შორის.

როგორ ჩავდგათ ტრაქეის მილი მოზრდილებში ლარინგოსკოპის გამოყენებით.

როგორ გამოვიყენოთ ნიღბიანი სასუნთქი ტომარა მოზრდილებთან ვენტილაციის უზრუნვესაყოფად. ვიდეო გვიჩვენებს ორი-პერსონის ტექნიკას.
გადაუდებელი ქირურგიული ჩარევა
მკურნალობა, რომელიც რეკომენდებულია <strong>ყველა</strong> პაციენტისთვის შერჩეულ ჯგუფში
კარდიოლოგიის ამერიკული კოლეჯი/ამერიკული გულის ასოციაცია (ACC/AHA) რეკომენდაციას უწევს კომპიუტერულ ტომოგრაფიას (CT) იმ პაციენტებში, რომლებსაც აღენიშნებათ გაგლეჯილი AAA, რომლებიც არიან ჰემოდინამიკურად სტაბილური, რათა შეაფასონ, ექვემდებარება თუ არა AAA ენდოვასკულარულ შეკეთებას.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com ეს რეკომენდაცია მხარდაჭერილია IMPROVE მრავალცენტრიანი რანდომიზებული კონტროლირებადი კვლევის შედეგებით, რომლებიც ვარაუდობენ, რომ პაციენტების უმეტესობისთვის დამადასტურებელი CT არ აფერხებდა მკურნალობის მიმდინარეობას და ხელს უწყობდა შესაბამის პრეოპერაციულ დაგეგმვას.[110]Powell JT, Hinchcliffe RJ, Thompson MM, et al; IMPROVE Trial Investigators. Observations from the IMPROVE trial concerning the clinical care of patients with ruptured abdominal aortic aneurysm. Br J Surg. 2014 Feb;101(3):216-24. https://bjssjournals.onlinelibrary.wiley.com/doi/full/10.1002/bjs.9410 http://www.ncbi.nlm.nih.gov/pubmed/24469620?tool=bestpractice.com
თუ ანატომია შესაბამისია, ACC/AHA რეკომენდაციას უწევს ენდოვასკულარულ ჩარევას, ღია პლასტიკის ნაცვლად, რათა შემცირდეს ავადობისა და სიკვდილიანობის რისკი.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com თუ პაციენტს დადასტურებული აქვს გახეთქილი მუცლის აორტის ანევრიზმა, ოპერაციის შემდეგ 3 წელიწადში სიკვდილობა უფრო დაბალია ენდოვასკულარული მიდგომის (EVAR) ჯგუფში, ვიდრე ღია მიდგომის ჯგუფში (48% vs. 56%; საფრთხის თანაფარდობა [HR] 0.57, 95% სარწმუნოობის ინტერვალი 0.36 - 0.90).[111]IMPROVE Trial Investigators. Comparative clinical effectiveness and cost effectiveness of endovascular strategy v open repair for ruptured abdominal aortic aneurysm: three year results of the IMPROVE randomised trial. BMJ. 2017 Nov 14;359:j4859. https://www.bmj.com/content/359/bmj.j4859.long http://www.ncbi.nlm.nih.gov/pubmed/29138135?tool=bestpractice.com განსხვავება სამკურნალო ჯგუფებს შორის აღარ იყო გამოხატული 7-წლიანი მეთვალყურეობის შემდეგ (HR 0.92, 95% CI 0.75 - 1.13). ხელახალი ჩარევის საჭიროების სიხშირე მნიშვნელოვნად არ განსხვავდებოდა რანდომიზებულ ჯგუფებს შორის 3 წლის შემდეგ (HR 1.02, 95% CI 0.79 - 1.32).[111]IMPROVE Trial Investigators. Comparative clinical effectiveness and cost effectiveness of endovascular strategy v open repair for ruptured abdominal aortic aneurysm: three year results of the IMPROVE randomised trial. BMJ. 2017 Nov 14;359:j4859. https://www.bmj.com/content/359/bmj.j4859.long http://www.ncbi.nlm.nih.gov/pubmed/29138135?tool=bestpractice.com არსებობს გარკვეული მტკიცებულება, რომ გაგლეჯილი მუცლის აორტის ანევრიზმის ენდოვასკულური სტრატეგიით ოპერირება ამცირებს სიკვდილობას უფრო ეფექტურად ქალებში, ვიდრე მამაკაცებში.[111]IMPROVE Trial Investigators. Comparative clinical effectiveness and cost effectiveness of endovascular strategy v open repair for ruptured abdominal aortic aneurysm: three year results of the IMPROVE randomised trial. BMJ. 2017 Nov 14;359:j4859. https://www.bmj.com/content/359/bmj.j4859.long http://www.ncbi.nlm.nih.gov/pubmed/29138135?tool=bestpractice.com [112]Sweeting MJ, Balm R, Desgranges P, et al; Ruptured Aneurysm Trialists. Individual-patient meta-analysis of three randomized trials comparing endovascular versus open repair for ruptured abdominal aortic aneurysm. Br J Surg. 2015 Sep;102(10):1229-39. https://bjssjournals.onlinelibrary.wiley.com/doi/full/10.1002/bjs.9852 http://www.ncbi.nlm.nih.gov/pubmed/26104471?tool=bestpractice.com
არსებობს გარკვეული მტკიცებულებები, რომლებიც ვარაუდობენ, რომ ანესთეზიის რეჟიმი AAA-ს ოპერაციული ჩარევის დროს გავლენას ახდენს შედეგებზე.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [113]Armstrong RA, Squire YG, Rogers CA, et al. Type of anesthesia for endovascular abdominal aortic aneurysm repair. J Cardiothorac Vasc Anesth. 2019 Feb;33(2):462-71. http://www.ncbi.nlm.nih.gov/pubmed/30342821?tool=bestpractice.com მულტიცენტრული რანდომიზებული კონტროლირებული კვლევამ IMPROVE გამოავლინა 30 დღიანი სიკვდილიანობის მნიშვნელოვანი შემცირება პაციენტებში, რომლებსაც ჩაუტარდათ EVAR тმხოლოდ ადგილობრივი ანესთეზიით, ზოგადი ანესთეზიის ქვეშ მყოფ პაციენტებთან შედარებით.(კორექტირებული OR 0,27 0,1-დან 0,7-მდე).[110]Powell JT, Hinchcliffe RJ, Thompson MM, et al; IMPROVE Trial Investigators. Observations from the IMPROVE trial concerning the clinical care of patients with ruptured abdominal aortic aneurysm. Br J Surg. 2014 Feb;101(3):216-24. https://bjssjournals.onlinelibrary.wiley.com/doi/full/10.1002/bjs.9410 http://www.ncbi.nlm.nih.gov/pubmed/24469620?tool=bestpractice.com ცალკეულმა მეტა-ანალიზმა, რომელიც ადარებს ანესთეზიის რეჟიმს გახეთქილი AAA-ს ენდოვასკულარული აღდგენისთვის, გაიმეორა ეს დასკვნები ან გააუმჯობესა შედეგები EVAR-ით ადგილობრივი ანესთეზიის ქვეშ.[114]Harky A, Ahmad MU, Santoro G, et al. Local versus general anesthesia in nonemergency endovascular abdominal aortic aneurysm repair: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth. 2020 Apr;34(4):1051-9. http://www.ncbi.nlm.nih.gov/pubmed/31473112?tool=bestpractice.com თუმცა, სხვა სისტემურმა მიმოხილვამ არ აჩვენა რაიმე სარგებელი სიკვდილიანობის შესახებ ადგილობრივი ანესთეზიით, მაგრამ აჩვენა სტაციონარული მკურნალობის უფრო ხანმოკლე პერიოდი.[115]Deng J, Liu J, Rong D, et al. A meta-analysis of locoregional anesthesia versus general anesthesia in endovascular repair of ruptured abdominal aortic aneurysm. J Vasc Surg. 2021 Feb;73(2):700-10. https://www.doi.org/10.1016/j.jvs.2020.08.112 http://www.ncbi.nlm.nih.gov/pubmed/32882348?tool=bestpractice.com
პერიოპერაციული ანტიბიოტიკოთერაპია
მკურნალობა, რომელიც რეკომენდებულია <strong>ყველა</strong> პაციენტისთვის შერჩეულ ჯგუფში
ანტიბიოტიკოთერაპია ნაჩვენებია იმ პაციენტებთან, რომელთაც უტარდებათ გადაუდებელი ქირურგიული ჩარევა მუცლის აორტის ანევრიზმის გასკდომის გამო, რათა გადაიფაროს გრამ-დადებითი და გრამ-უარყოფითი ფლორა და თავიდან იქნას აცილებული გრაფტის ინფექცია.
ფართო სპექტრის ანტიბიოტიკებით დაფარვა მორგებულია კლინიკური გამოვლინებაზე და ბაქტერიოლოგიური კვლევის შედეგებზე, და შეესაბამება ადგილობრივ პროტოკოლებს.
ინფექციურ-ანთებითი პროცესების მკურნალობა.
დამატებითი მკურნალობა, რომელიც რეკომენდებულია <strong>ზოგიერთი</strong> პაციენტისთვის შერჩეული ჯგუფიდან
მას შემდეგ, რაც პაციენტი სტაბილურია და გასკდომის სასწრაფო ქირურგიული ჩარევა იქნება პრიორიტეტული, უნდა განიხილებოდეს ინფექციური ან ანთებითი ეტიოლოგია.
თუ პაციენტს აქვს საეჭვო ინფექციური ანევრიზმა, ადრეული დიაგნოსტიკა და დროული მკურნალობა აუცილებელია შედეგების გასაუმჯობესებლად.[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com ამ პაციენტებში გადაუდებელი ქირურგიული ჩარევის დროს ხშირად საჭირო ხდება ფართო სანაცია. არსებობს მეორადი ინფექციური გართულებების მაღალი რისკი და შეიძლება საჭირო გახდეს შემდგომი ოპერაცია ახალი ინფექციური დაზიანებისთვის. ინტრაოპერაციული კულტურები უნდა იქნას მიღებული შემდგომი ანტიბიოტიკოთერაპიის სწორად წარმართვისთვის; თუმცა, ემპირიული ანტიბიოტიკები ხშირად ინიშნება, რადგან პერიფერიული სისხლის კულტურები და ქირურგიული ნიმუშების კულტურები ნეგატიურია პაციენტთა დიდ ნაწილში.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com შესაძლოა ნაჩვენები იყოს ხანგრძლივი ანტიბიოტიკოთერაპია (4-6 კვირიდან სიცოცხლის ხანგრძლივ პერიოდში) სპეციფიკური პათოგენის, ოპერაციული პლასტიკის ტიპისა და პაციენტის იმუნოლოგიური მდგომარეობის მიხედვით.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
ანთებითი აორტიტის დროს (გამოწვეული, მაგალითად, ტაკაიასუს არტერიტით ან გიგანტურუჯრედოვანი არტერიტით) მკურნალობა ხდება კორტიკოსტეროიდების მაღალი დოზით და ქირურგიული ჩარევით.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [200]Ben Jmaà H, Karray R, Jmal H, et al. Surgical and endoluminal management of the inflammatory aortitis: a Tunisian center experience [in French]. J Med Vasc. 2017 Jul;42(4):213-20. http://www.ncbi.nlm.nih.gov/pubmed/28705339?tool=bestpractice.com
სიმპტომური, მაგრამ არა გამსკდარი მუცლის აორტის ანევრიზმი
გადაუდებელი ქირურგიული ჩარევა
პაციენტებისათვის, რომელთაც აღენიშნებათ სიმპტომური აორტის ანევრიზმა, მკურნალობა ნაჩვენებია მიუხედავად აორტის დიამეტრისა.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [67]National Institute for Health and Care Excellence. Abdominal aortic aneurysm: diagnosis and management. Mar 2020 [internet publication]. https://www.nice.org.uk/guidance/ng156 [122]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926. https://academic.oup.com/eurheartj/article/35/41/2873/407693 http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com ახლად აღმოცენებული ტკივილი ან ტკივილის გაუარესება შეიძლება მიანიშნებდეს ანევრიზმის გაფართოებაზე ან მოსალოდნელ გაგლეჯაზე. სიმპტომური, მთლიანი ანევრიზმის მკურნალობა ურგენტულადაა რეკომენდებული.[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2. https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com ზოგიერთ შემთხვევაში ოპერაციისათვის ოპტიმალური პირობების შესაქმნელად, ჩარევა შეიძლება რამდენიმე საათით გადაიდოს; ამ პაციენტების მონიტორინგი რეკომენდებულია ინტენსიურ განყოფილებაში.[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2. https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com
EVAR უფრო და უფრო ხშირად გამოიყენება სიმპტომური მუცლის აორტის ანევრიზმის სამართავად.[123]De Martino RR, Nolan BW, Goodney PP, Chang CK, et al; Vascular Study Group of Northern New England. Outcomes of symptomatic abdominal aortic aneurysm repair. J Vasc Surg. 2010 Jul;52(1):5-12.e1. https://www.jvascsurg.org/article/S0741-5214(10)00259-4/fulltext http://www.ncbi.nlm.nih.gov/pubmed/20471771?tool=bestpractice.com [124]Chandra V, Trang K, Virgin-Downey W, et al. Management and outcomes of symptomatic abdominal aortic aneurysms during the past 20 years. J Vasc Surg. 2017 Dec;66(6):1679-85. http://www.ncbi.nlm.nih.gov/pubmed/28619644?tool=bestpractice.com ობსერვაციული კვლევების თანახმად, მოკლევადიანი, ნებისმიერი მიზეზით განპირობებული სიკვდილობის სიხშირე არ განსხვავდებოდა ენდოვასკულურ და ღია მეთოდებს შორის სიმპტომური ანევრიზმის დროს.[123]De Martino RR, Nolan BW, Goodney PP, Chang CK, et al; Vascular Study Group of Northern New England. Outcomes of symptomatic abdominal aortic aneurysm repair. J Vasc Surg. 2010 Jul;52(1):5-12.e1. https://www.jvascsurg.org/article/S0741-5214(10)00259-4/fulltext http://www.ncbi.nlm.nih.gov/pubmed/20471771?tool=bestpractice.com [124]Chandra V, Trang K, Virgin-Downey W, et al. Management and outcomes of symptomatic abdominal aortic aneurysms during the past 20 years. J Vasc Surg. 2017 Dec;66(6):1679-85. http://www.ncbi.nlm.nih.gov/pubmed/28619644?tool=bestpractice.com [125]Ten Bosch JA, Willigendael EM, Kruidenier LM, et al. Early and mid-term results of a prospective observational study comparing emergency endovascular aneurysm repair with open surgery in both ruptured and unruptured acute abdominal aortic aneurysms. Vascular. 2012 Apr;20(2):72-80. http://www.ncbi.nlm.nih.gov/pubmed/22454547?tool=bestpractice.com
პერიოპერაციული კარდიოვასკულარული რისკის შემცირება
მკურნალობა, რომელიც რეკომენდებულია <strong>ყველა</strong> პაციენტისთვის შერჩეულ ჯგუფში
ცვლადი გულსისხლძარღვთა რისკფაქტორების კონტროლი პრეოპერაციულად აუმჯობესებს ჩარევის შემდგომ გადარჩენის სიხშირეს.[190]Khashram M, Williman JA, Hider PN, et al. Management of modifiable vascular risk factors improves late survival following abdominal aortic aneurysm repair: a systematic review and meta-analysis. Ann Vasc Surg. 2017 Feb;39:301-11. http://www.ncbi.nlm.nih.gov/pubmed/27666804?tool=bestpractice.com
წინასაოპერაციო ვარჯიშმა ფიზიკური დატვირთვით დააქვეითა პოსტოპერაციული კარდიალური გართულებები მცირე რანდომიზებული კონტროლირებადი კვლევების მიხედვით.პაციენტებში,რომლებმაც გადაიტანეს ღია ან ენდოვასკულარული AAA პლასტიკა, თუმცა კოხრეინის მიმოხილვამ და ოპერაციამდე პრეჰაბილიტაციის (სავარჯიშო ტრენინგის) ცალკეული სისტემატური მიმოხილვამ არ აჩვენა რაიმე შედეგის სარგებელი.[191]Barakat HM, Shahin Y, Khan JA, et al. Preoperative supervised exercise improves outcomes after elective abdominal aortic aneurysm repair: a randomized controlled trial. Ann Surg. 2016 Jul;264(1):47-53. http://www.ncbi.nlm.nih.gov/pubmed/26756766?tool=bestpractice.com [192]Fenton C, Tan AR, Abaraogu UO, et al. Prehabilitation exercise therapy before elective abdominal aortic aneurysm repair. Cochrane Database Syst Rev. 2021 Jul 8;7(7):CD013662. https://www.doi.org/10.1002/14651858.CD013662.pub2 http://www.ncbi.nlm.nih.gov/pubmed/34236703?tool=bestpractice.com [193]Bonner RJ, Wallace T, Jones AD, et al. The content of pre-habilitative interventions for patients undergoing repair of abdominal aortic aneurysms and their effect on post-operative outcomes: a systematic review. Eur J Vasc Endovasc Surg. 2021 May;61(5):756-65. https://www.doi.org/10.1016/j.ejvs.2021.01.043 http://www.ncbi.nlm.nih.gov/pubmed/33678532?tool=bestpractice.com მიუხედავად იმისა, რომ წინასაოპერაციო ვარჯიში შეიძლება სასარგებლო იყოს პაციენტებისთვის, რომლებიც გადიან AAA-ს პლასტიკას, საჭიროა შემდგომი გამოკვლევა RCT-ებით, სანამ ის უფრო ფართოდ იქნება რეკომენდებული.[194]Wee IJY, Choong AMTL. A systematic review of the impact of preoperative exercise for patients with abdominal aortic aneurysm. J Vasc Surg. 2020 Jun;71(6):2123-31.e1. https://www.doi.org/10.1016/j.jvs.2018.09.039 http://www.ncbi.nlm.nih.gov/pubmed/30606665?tool=bestpractice.com
პერიოპერაციული სტატინების გამოყენება ანელებს ანევრიზმის ზრდას, ამცირებს რღვევის რისკს და ამცირებს სიკვდილიანობას AAA-ს პლასტიკის ან გახეთქილი AAA-სგან.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com სტატინები უნდა დაინიშნოს ქირურგიულ ჩარევამდე სულ მცირე 1 თვით ადრე, რათა შემცირდეს გულსისხლძარღვთა მიზეზით სიკვდილობა. სტატინები გრძელდება განუსაზღვრელი ვადით.[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com [136]Risum Ø, Sandven I, Sundhagen JO, et al. Editor's choice - effect of statins on total mortality in abdominal aortic aneurysm repair: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2021 Jan;61(1):114-20. https://www.doi.org/10.1016/j.ejvs.2020.08.007 http://www.ncbi.nlm.nih.gov/pubmed/32928667?tool=bestpractice.com
პაციენტებს AAA-ით აქვთ მაღალი რისკი გულ-სისხლძარღვთა დაავადებების სერიოზული გართულებების მხრივ. არსებობს შეზღუდული მტკიცებულება, მაგრამ რაიმე უკუჩვენების არარსებობის შემთხვევაში, AAA-ს მქონე პაციენტებმა უნდა მიიღონ ერთჯერადი ანტითრომბოციტული თერაპია (ასპირინი ან კლოპიდოგრელი).[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [137]Aboyans V, Bauersachs R, Mazzolai L, et al. Antithrombotic therapies in aortic and peripheral arterial diseases in 2021: a consensus document from the ESC working group on aorta and peripheral vascular diseases, the ESC working group on thrombosis, and the ESC working group on cardiovascular pharmacotherapy. Eur Heart J. 2021 Oct 14;42(39):4013-24. https://www.doi.org/10.1093/eurheartj/ehab390 http://www.ncbi.nlm.nih.gov/pubmed/34279602?tool=bestpractice.com დააკვირდეთ პაციენტებს პერიოპერაციულ პერიოდში[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
ჰიპერტენზია უნდა გაკონტროლდეს გულსისხლძარღვთა ავადობის შესამცირებლად.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
პრეოპერაციული კურსი ბეტა-ბლოკერებით შეიძლება გამართლებული იყოს პაციენტებში, რომელთაც მიოკარდიუმის იშემიის მაღალი რისკი აქვთ (გულის იშემიური დაავადება ან მიუკარდიუმის იშემია სტრეს-ტესტზე). თერაპია ქირურგიულ ჩარევამდე 1 თვით ადრე უნდა ჩატარდეს.[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com [195]Chen RJ, Chu H, Tsai LW. Impact of beta-blocker initiation timing on mortality risk in patients with diabetes mellitus undergoing noncardiac surgery: a nationwide population-based cohort study. J Am Heart Assoc. 2017 Jan 10;6(1):e004392. https://www.ahajournals.org/doi/full/10.1161/jaha.116.004392 http://www.ncbi.nlm.nih.gov/pubmed/28073770?tool=bestpractice.com ფართომასშტაბიან კვლევებში, რომლებშიც ბეტა ბლოკერი ქირურგიულ ჩარევამდე რამდენიმე დღით ადრე დაიწყოს, პერიოპერაციულად ბეტა ბლოკერის სარგებელი ან ზიანი არ გამოვლინდა.[196]Brady AR, Gibbs JS, Greenhalgh RM, et al; POBBLE Trial Investigators. Perioperative beta-blockade (Pobble) for patients undergoing infrarenal vascular surgery: results of a randomized double-blind controlled trial. J Vasc Surg. 2005 Apr;41(4):602-9. https://www.jvascsurg.org/article/S0741-5214(05)00189-8/fulltext http://www.ncbi.nlm.nih.gov/pubmed/15874923?tool=bestpractice.com [197]Devereaux PJ, Yang H, Yusuf S, et al; POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008 May 31;371(9627):1839-47. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(08)60601-7/fulltext http://www.ncbi.nlm.nih.gov/pubmed/18479744?tool=bestpractice.com [198]Yang H, Raymer K, Butler R, et al. The effects of perioperative beta-blockade: results of the Metoprolol after Vascular Surgery (MaVS) study, a randomized controlled trial. Am Heart J. 2006 Nov;152(5):983-90. http://www.ncbi.nlm.nih.gov/pubmed/17070177?tool=bestpractice.com
პერიოპერაციული ანტიბიოტიკოთერაპია
მკურნალობა, რომელიც რეკომენდებულია <strong>ყველა</strong> პაციენტისთვის შერჩეულ ჯგუფში
ჩაუტარდა პერიოპერაციული ანტიბიოტიკოთერაპია. ფართო სპექტრის ანტიბიოტიკებით პროფილაქტიკა აუცილებელია, ადგილობრივი პროტოკოლის თანახმად.
ინფექციურ-ანთებითი პროცესების მკურნალობა.
დამატებითი მკურნალობა, რომელიც რეკომენდებულია <strong>ზოგიერთი</strong> პაციენტისთვის შერჩეული ჯგუფიდან
მას შემდეგ, რაც პაციენტი სტაბილურია და გასკდომის სასწრაფო ქირურგიული ჩარევა იქნება პრიორიტეტული, უნდა განიხილებოდეს ინფექციური ან ანთებითი ეტიოლოგია.
თუ პაციენტს აქვს საეჭვო ინფექციური ანევრიზმა, ადრეული დიაგნოსტიკა და დროული მკურნალობა აუცილებელია შედეგების გასაუმჯობესებლად.[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com ამ პაციენტებში გადაუდებელი ქირურგიული ჩარევის დროს ხშირად საჭირო ხდება ფართო სანაცია. არსებობს მეორადი ინფექციური გართულებების მაღალი რისკი და შეიძლება საჭირო გახდეს შემდგომი ოპერაცია ახალი ინფექციური დაზიანებისთვის. ინტრაოპერაციული კულტურები უნდა იქნას მიღებული შემდგომი ანტიბიოტიკოთერაპიის სწორად წარმართვისთვის; თუმცა, ემპირიული ანტიბიოტიკები ხშირად ინიშნება, რადგან პერიფერიული სისხლის კულტურები და ქირურგიული ნიმუშების კულტურები ნეგატიურია პაციენტთა დიდ ნაწილში.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com შესაძლოა ნაჩვენები იყოს ხანგრძლივი ანტიბიოტიკოთერაპია (4-6 კვირიდან სიცოცხლის ხანგრძლივ პერიოდში) სპეციფიკური პათოგენის, ოპერაციული პლასტიკის ტიპისა და პაციენტის იმუნოლოგიური მდგომარეობის მიხედვით.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
ანთებითი აორტიტის დროს (გამოწვეული, მაგალითად, ტაკაიასუს არტერიტით ან გიგანტურუჯრედოვანი არტერიტით) მკურნალობა ხდება კორტიკოსტეროიდების მაღალი დოზით და ქირურგიული ჩარევით.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [200]Ben Jmaà H, Karray R, Jmal H, et al. Surgical and endoluminal management of the inflammatory aortitis: a Tunisian center experience [in French]. J Med Vasc. 2017 Jul;42(4):213-20. http://www.ncbi.nlm.nih.gov/pubmed/28705339?tool=bestpractice.com
შემთხვევითი აღმოჩენა: მცირე ზომის მუცლის აორტის ანევრიზმა
ზედამხედველობა
პაციენტებში, რომელთაც მუცლის აორტის ანევრიზმა დაუდგინდათ შემთხვევით, უპირატესია დაკვირვება ქირურგიულ ჩარევასთან შედარებით მანამ, სანამ გასკდომის რისკი არ გადააჭარბებს ოპერაციის შემდგომი სიკვდილობის რისკს.[3]Owens DK, Davidson KW, Krist AH, et al; US Preventive Services Task Force. Screening for abdominal aortic aneurysm: US Preventive Services Task Force recommendation statement. JAMA. 2019 Dec 10;322(22):2211-8. https://jamanetwork.com/journals/jama/fullarticle/2757234 http://www.ncbi.nlm.nih.gov/pubmed/31821437?tool=bestpractice.com [122]Erbel R, Aboyans V, Boileau C, et al; ESC Committee for Practice Guidelines. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014 Nov 1;35(41):2873-926. https://academic.oup.com/eurheartj/article/35/41/2873/407693 http://www.ncbi.nlm.nih.gov/pubmed/25173340?tool=bestpractice.com
მუცლის აორტის უფრო მცირე ზომის ანევრიზმების ადრეული ღია ქირურგიული მკურნალობა არ ამცირებს ნებისმიერი მიზეზით ან ანევრიზმით გამოწვეულ სიკვდილობას.[3]Owens DK, Davidson KW, Krist AH, et al; US Preventive Services Task Force. Screening for abdominal aortic aneurysm: US Preventive Services Task Force recommendation statement. JAMA. 2019 Dec 10;322(22):2211-8.
https://jamanetwork.com/journals/jama/fullarticle/2757234
http://www.ncbi.nlm.nih.gov/pubmed/31821437?tool=bestpractice.com
[127]Ulug P, Powell JT, Martinez MA, et al. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database Syst Rev. 2020 Jul 1;7(7):CD001835.
https://www.doi.org/10.1002/14651858.CD001835.pub5
http://www.ncbi.nlm.nih.gov/pubmed/32609382?tool=bestpractice.com
[ ![]() ]
How does immediate surgery compare with surveillance in people with asymptomatic abdominal aortic aneurysms (AAAs)?/cca.html?targetUrl=https://www.cochranelibrary.com/cca/doi/10.1002/cca.3227/fullსწორი პასუხის ჩვენებაერთ-ერთი სისტემური მიმოხილვის თანახმად (4 კვლევა, 3314 მონაწილე), არსებობს მაღალი ხარისხის მტკიცებულება, რომ მცირე ზომის AAA(4 სმ- 5.5 სმ) მუცლის აორტის ანევრიზმის ოპერაცია გრძელვადიანი გადარჩენის თვალსაზრისით, დაკვირვებით ტაქტიკასთან შედარებით(კორეგირებული საფრთხის თანაფარდობა 0.88, 95% სარწმუნოობის ინტერვალი 0.75 - 1.02, საშუალოდ 10 წელი შემდგომი დაკვირვებით) არაეფექტურია.[127]Ulug P, Powell JT, Martinez MA, et al. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database Syst Rev. 2020 Jul 1;7(7):CD001835.
https://www.doi.org/10.1002/14651858.CD001835.pub5
http://www.ncbi.nlm.nih.gov/pubmed/32609382?tool=bestpractice.com
დაუყოვნებლივი ქირურგიულ ჩარევის დაბალი სარგებლიანობა ვლინდებოდა ყველა ასაკში, მცირე ზომის ანევრიზმის ნებისმიერ დიამეტრზე და ენდოვასკულური/ღია მეთოდების ჯგუფებშიც.[127]Ulug P, Powell JT, Martinez MA, et al. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database Syst Rev. 2020 Jul 1;7(7):CD001835.
https://www.doi.org/10.1002/14651858.CD001835.pub5
http://www.ncbi.nlm.nih.gov/pubmed/32609382?tool=bestpractice.com
]
How does immediate surgery compare with surveillance in people with asymptomatic abdominal aortic aneurysms (AAAs)?/cca.html?targetUrl=https://www.cochranelibrary.com/cca/doi/10.1002/cca.3227/fullსწორი პასუხის ჩვენებაერთ-ერთი სისტემური მიმოხილვის თანახმად (4 კვლევა, 3314 მონაწილე), არსებობს მაღალი ხარისხის მტკიცებულება, რომ მცირე ზომის AAA(4 სმ- 5.5 სმ) მუცლის აორტის ანევრიზმის ოპერაცია გრძელვადიანი გადარჩენის თვალსაზრისით, დაკვირვებით ტაქტიკასთან შედარებით(კორეგირებული საფრთხის თანაფარდობა 0.88, 95% სარწმუნოობის ინტერვალი 0.75 - 1.02, საშუალოდ 10 წელი შემდგომი დაკვირვებით) არაეფექტურია.[127]Ulug P, Powell JT, Martinez MA, et al. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database Syst Rev. 2020 Jul 1;7(7):CD001835.
https://www.doi.org/10.1002/14651858.CD001835.pub5
http://www.ncbi.nlm.nih.gov/pubmed/32609382?tool=bestpractice.com
დაუყოვნებლივი ქირურგიულ ჩარევის დაბალი სარგებლიანობა ვლინდებოდა ყველა ასაკში, მცირე ზომის ანევრიზმის ნებისმიერ დიამეტრზე და ენდოვასკულური/ღია მეთოდების ჯგუფებშიც.[127]Ulug P, Powell JT, Martinez MA, et al. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database Syst Rev. 2020 Jul 1;7(7):CD001835.
https://www.doi.org/10.1002/14651858.CD001835.pub5
http://www.ncbi.nlm.nih.gov/pubmed/32609382?tool=bestpractice.com
მცირე ზომის ანევრიზმების დროს ქირურგიული ჩარევა რეკომენდებულია თუ ანევრიზმა სწრაფად იზრდება ან ანევრიზმის ქირურგიული ზღვრული მაჩვენებელი მიღწეულია განმეორებითი ულტრაბგერის კვლევაზე.[3]Owens DK, Davidson KW, Krist AH, et al; US Preventive Services Task Force. Screening for abdominal aortic aneurysm: US Preventive Services Task Force recommendation statement. JAMA. 2019 Dec 10;322(22):2211-8. https://jamanetwork.com/journals/jama/fullarticle/2757234 http://www.ncbi.nlm.nih.gov/pubmed/31821437?tool=bestpractice.com
კარდიოვასკულური რისკების აგრესიული მართვა
მკურნალობა, რომელიც რეკომენდებულია <strong>ყველა</strong> პაციენტისთვის შერჩეულ ჯგუფში
ცვლადი გულსისხლძარღვთა რისკფაქტორების კონტროლი პრეოპერაციულად აუმჯობესებს ჩარევის შემდგომ გადარჩენის სიხშირეს.[190]Khashram M, Williman JA, Hider PN, et al. Management of modifiable vascular risk factors improves late survival following abdominal aortic aneurysm repair: a systematic review and meta-analysis. Ann Vasc Surg. 2017 Feb;39:301-11. http://www.ncbi.nlm.nih.gov/pubmed/27666804?tool=bestpractice.com
პაციენტებს უნდა მიეცეთ რეკომენდაცია მოწევის შეწყვეტასთან დაკავშირებით და უნდა შესთავაზონ, საჭიროების შემთხვევაში, მედიკამენტური მკურნალობა.[1]Dehlin JM, Upchurch GR. Management of abdominal aortic aneurysms. Curr Treat Options Cardiovasc Med. 2005 Jun;7(2):119-30.
http://www.ncbi.nlm.nih.gov/pubmed/15935120?tool=bestpractice.com
[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482.
https://www.doi.org/10.1161/CIR.0000000000001106
http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com
[13]Zankl AR, Schumacher H, Krumsdorf U, et al. Pathology, natural history and treatment of abdominal aortic aneurysms. Clin Res Cardiol. 2007 Mar;96(3):140-51.
http://www.ncbi.nlm.nih.gov/pubmed/17180573?tool=bestpractice.com
[15]Singh K, Bønaa H, Jacobsen BK, et al. Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study: the Tromsø Study. Am J Epidemiol. 2001 Aug 1;154(3):236-44.
https://academic.oup.com/aje/article/154/3/236/125840
http://www.ncbi.nlm.nih.gov/pubmed/11479188?tool=bestpractice.com
[23]Lederle FA, Johnson GR, Wilson SE, et al; Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Prevalence and associations of abdominal aortic aneurysm detected through screening. Ann Intern Med. 1997 Mar 15;126(6):441-9.
http://www.ncbi.nlm.nih.gov/pubmed/9072929?tool=bestpractice.com
[24]Wilmink TB, Quick CR, Day NE. The association between cigarette smoking and abdominal aortic aneurysms. J Vasc Surg. 1999 Dec;30(6):1099-105.
http://www.ncbi.nlm.nih.gov/pubmed/10587395?tool=bestpractice.com
[131]Hartmann-Boyce J, Chepkin SC, Ye W, et al. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst Rev. 2018 May 31;5:CD000146.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000146.pub5/full
http://www.ncbi.nlm.nih.gov/pubmed/29852054?tool=bestpractice.com
[132]Rigotti NA, Clair C, Munafò MR, et al. Interventions for smoking cessation in hospitalised patients. Cochrane Database Syst Rev. 2012 May 16;(5):CD001837.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001837.pub3/full
http://www.ncbi.nlm.nih.gov/pubmed/22592676?tool=bestpractice.com
[133]Howes S, Hartmann-Boyce J, Livingstone-Banks J, et al. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2020 Apr 22;(4):CD000031.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000031.pub5/full
http://www.ncbi.nlm.nih.gov/pubmed/32319681?tool=bestpractice.com
[ ![]() ]
What are the effects of adding bupropion or fluoxetine to other treatments compared with using other treatments alone for people trying to quit smoking?/cca.html?targetUrl=https://www.cochranelibrary.com/cca/doi/10.1002/cca.4337/fullსწორი პასუხის ჩვენება
]
What are the effects of adding bupropion or fluoxetine to other treatments compared with using other treatments alone for people trying to quit smoking?/cca.html?targetUrl=https://www.cochranelibrary.com/cca/doi/10.1002/cca.4337/fullსწორი პასუხის ჩვენება
წინასაოპერაციო ვარჯიშმა ფიზიკური დატვირთვით დააქვეითა პოსტოპერაციული კარდიალური გართულებები მცირე რანდომიზებული კონტროლირებადი კვლევების მიხედვით.პაციენტებში,რომლებმაც გადაიტანეს ღია ან ენდოვასკულარული AAA პლასტიკა, თუმცა კოხრეინის მიმოხილვამ და ოპერაციამდე პრეჰაბილიტაციის (სავარჯიშო ტრენინგის) ცალკეული სისტემატური მიმოხილვამ არ აჩვენა რაიმე შედეგის სარგებელი.[191]Barakat HM, Shahin Y, Khan JA, et al. Preoperative supervised exercise improves outcomes after elective abdominal aortic aneurysm repair: a randomized controlled trial. Ann Surg. 2016 Jul;264(1):47-53. http://www.ncbi.nlm.nih.gov/pubmed/26756766?tool=bestpractice.com [192]Fenton C, Tan AR, Abaraogu UO, et al. Prehabilitation exercise therapy before elective abdominal aortic aneurysm repair. Cochrane Database Syst Rev. 2021 Jul 8;7(7):CD013662. https://www.doi.org/10.1002/14651858.CD013662.pub2 http://www.ncbi.nlm.nih.gov/pubmed/34236703?tool=bestpractice.com [193]Bonner RJ, Wallace T, Jones AD, et al. The content of pre-habilitative interventions for patients undergoing repair of abdominal aortic aneurysms and their effect on post-operative outcomes: a systematic review. Eur J Vasc Endovasc Surg. 2021 May;61(5):756-65. https://www.doi.org/10.1016/j.ejvs.2021.01.043 http://www.ncbi.nlm.nih.gov/pubmed/33678532?tool=bestpractice.com მიუხედავად იმისა, რომ წინასაოპერაციო ვარჯიში შეიძლება სასარგებლო იყოს პაციენტებისთვის, რომლებიც გადიან AAA-ს პლასტიკას, საჭიროა შემდგომი გამოკვლევა RCT-ებით, სანამ ის უფრო ფართოდ იქნება რეკომენდებული.[194]Wee IJY, Choong AMTL. A systematic review of the impact of preoperative exercise for patients with abdominal aortic aneurysm. J Vasc Surg. 2020 Jun;71(6):2123-31.e1. https://www.doi.org/10.1016/j.jvs.2018.09.039 http://www.ncbi.nlm.nih.gov/pubmed/30606665?tool=bestpractice.com
პერიოპერაციული სტატინების გამოყენება ანელებს ანევრიზმის ზრდას, ამცირებს რღვევის რისკს და ამცირებს სიკვდილიანობას AAA-ს პლასტიკის ან გახეთქილი AAA-სგან.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com სტატინები უნდა დაინიშნოს ქირურგიულ ჩარევამდე სულ მცირე 1 თვით ადრე, რათა შემცირდეს გულსისხლძარღვთა მიზეზით სიკვდილობა. სტატინები გრძელდება განუსაზღვრელი ვადით.[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com [136]Risum Ø, Sandven I, Sundhagen JO, et al. Editor's choice - effect of statins on total mortality in abdominal aortic aneurysm repair: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2021 Jan;61(1):114-20. https://www.doi.org/10.1016/j.ejvs.2020.08.007 http://www.ncbi.nlm.nih.gov/pubmed/32928667?tool=bestpractice.com
პაციენტებს AAA-ით აქვთ მაღალი რისკი გულ-სისხლძარღვთა დაავადებების სერიოზული გართულებების მხრივ. არსებობს შეზღუდული მტკიცებულება, მაგრამ რაიმე უკუჩვენების არარსებობის შემთხვევაში, AAA-ს მქონე პაციენტებმა უნდა მიიღონ ერთჯერადი ანტითრომბოციტული თერაპია (ასპირინი ან კლოპიდოგრელი).[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [137]Aboyans V, Bauersachs R, Mazzolai L, et al. Antithrombotic therapies in aortic and peripheral arterial diseases in 2021: a consensus document from the ESC working group on aorta and peripheral vascular diseases, the ESC working group on thrombosis, and the ESC working group on cardiovascular pharmacotherapy. Eur Heart J. 2021 Oct 14;42(39):4013-24. https://www.doi.org/10.1093/eurheartj/ehab390 http://www.ncbi.nlm.nih.gov/pubmed/34279602?tool=bestpractice.com დააკვირდეთ პაციენტებს პერიოპერაციულ პერიოდში[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
ჰიპერტენზია უნდა გაკონტროლდეს გულსისხლძარღვთა ავადობის შესამცირებლად.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
ინფექციურ-ანთებითი პროცესების მკურნალობა.
დამატებითი მკურნალობა, რომელიც რეკომენდებულია <strong>ზოგიერთი</strong> პაციენტისთვის შერჩეული ჯგუფიდან
უნდა განიხილებოდეს ინფექციური ან ანთებითი ეტიოლოგია.
თუ პაციენტს აქვს საეჭვო ინფექციური ანევრიზმა, ადრეული დიაგნოსტიკა, დროული მკურნალობა ანტიბიოტიკებით და სასწრაფო ქირურგიული ჩარევა აუცილებელია შედეგების გასაუმჯობესებლად.[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com ამ პაციენტებში გადაუდებელი ქირურგიული ჩარევის დროს ხშირად საჭირო ხდება ფართო სანაცია. არსებობს მეორადი ინფექციური გართულებების მაღალი რისკი და შეიძლება საჭირო გახდეს შემდგომი ოპერაცია ახალი ინფექციური დაზიანებისთვის. ინტრაოპერაციული კულტურები უნდა იქნას მიღებული შემდგომი ანტიბიოტიკოთერაპიის სწორად წარმართვისთვის; თუმცა, ემპირიული ანტიბიოტიკები ხშირად ინიშნება, რადგან პერიფერიული სისხლის კულტურები და ქირურგიული ნიმუშების კულტურები ნეგატიურია პაციენტთა დიდ ნაწილში.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com შესაძლოა ნაჩვენები იყოს ხანგრძლივი ანტიბიოტიკოთერაპია (4-6 კვირიდან სიცოცხლის ხანგრძლივ პერიოდში) სპეციფიკური პათოგენის, ოპერაციული პლასტიკის ტიპისა და პაციენტის იმუნოლოგიური მდგომარეობის მიხედვით.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
ანთებითი აორტიტის დროს (გამოწვეული, მაგალითად, ტაკაიასუს არტერიტით ან გიგანტურუჯრედოვანი არტერიტით) მკურნალობა ხდება კორტიკოსტეროიდების მაღალი დოზით და ქირურგიული ჩარევით.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [200]Ben Jmaà H, Karray R, Jmal H, et al. Surgical and endoluminal management of the inflammatory aortitis: a Tunisian center experience [in French]. J Med Vasc. 2017 Jul;42(4):213-20. http://www.ncbi.nlm.nih.gov/pubmed/28705339?tool=bestpractice.com
შემთხვევითი აღმოჩენა: მუცლის აორტის დიდი ზომის ანევრიზმა
ელექტიური ქირურგიული ჩარევა
ძირითადად, ქირურგიული მკურნალობა ნაჩვენებია მუცლის აორტის ანევრიზმის მქონე პაციენტებში, როდესაც ანევრიზმა დიდი ზომისაა (მაგ.: აშშ-ში მამაკაცებში დიამეტრი > 5.5 სმ, ხოლო ქალებში - >5.0 სმ), თუმცა, სხვა ქვეყნებში, მკურნალობის შესახებ გადაწყვეტილება მიიღება ანევრიზმის უფრო დიდი ზომის შემთხვევაში.[67]National Institute for Health and Care Excellence. Abdominal aortic aneurysm: diagnosis and management. Mar 2020 [internet publication]. https://www.nice.org.uk/guidance/ng156 ≥5.5 სმ ანევრიზმის ოპერირებით გადარჩენადობა უმჯობესდება.[1]Dehlin JM, Upchurch GR. Management of abdominal aortic aneurysms. Curr Treat Options Cardiovasc Med. 2005 Jun;7(2):119-30. http://www.ncbi.nlm.nih.gov/pubmed/15935120?tool=bestpractice.com [78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2. https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com [106]UK Small Aneurysm Trial Participants. Mortality results for randomized controlled trial of early elective surgery or ultrasonographic surveillance for small abdominal aortic aneurysms. Lancet. 1998 Nov 21;352(9141):1649-55. http://www.ncbi.nlm.nih.gov/pubmed/9853436?tool=bestpractice.com [107]Powell JT, Brady AR, Brown LC, et al; United Kingdom Small Aneurysm Trial Participants. Long-term outcomes of immediate repair compared with surveillance of small abdominal aortic aneurysms. N Engl J Med. 2002 May 9;346(19):1445-52. https://www.nejm.org/doi/full/10.1056/NEJMoa013527 http://www.ncbi.nlm.nih.gov/pubmed/12000814?tool=bestpractice.com [108]Powell JT, Brown LC, Forbes JF, et al. Final 12-year follow-up of surgery versus surveillance in the UK Small Aneurysm Trial. Br J Surg. 2007 Jun;94(6):702-8. http://www.ncbi.nlm.nih.gov/pubmed/17514693?tool=bestpractice.com
ქირურგიულ ჩარევასთან დაკავშირებული გადაწყვეტილებები ინდივიდუალურად უნდა იქნას მიღებული. გასათვალისწინებელია პაციენტის არჩევანი, ასაკი, სქესი, პერიოპერაციული რისკფაქტორები და ანტომიური რისკფაქტორები. გასათვალისწინებელია პაციენტის სიცოცხლის ხარისხი. პაციენტს უნდა აუხსნათ ჩარევის რისკები და გაესაუბროთ სიცოცხლის ოპერაციის შემდგომი ხარისხის შესახებ. რეკომენდებულია გადაწყვეტილების მიღების საერთო მიდგომა პროცედურების რისკებისა და სარგებლის გათვალისწინებით.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [127]Ulug P, Powell JT, Martinez MA, et al. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database Syst Rev. 2020 Jul 1;7(7):CD001835. https://www.doi.org/10.1002/14651858.CD001835.pub5 http://www.ncbi.nlm.nih.gov/pubmed/32609382?tool=bestpractice.com
მონაცემების თანახმად, დიდი ზომის (≥5.5 სმ) მუცლის აორტის ანევრიზმის მქონე პაციენტებს, რომელთაც უტარდებათ რეკომენდებული მკურნალობა, EVAR-ისა და ღია წესით ჩატარებული მკურნალობის გამოსავალი ერთნაირია გადარჩენის მიხედვით, თუმცა განმეორებითი ჩარევის სიხშირის მაჩვენებელი EVAR-ის შემთხვევაში უფრო მაღალია.[138]Greenhalgh RM, Brown LC, Powell JT, et al; United Kingdom EVAR Trial Investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010 May 20;362(20):1863-71. http://www.ncbi.nlm.nih.gov/pubmed/20382983?tool=bestpractice.com [139]Amato B, Fugetto F, Compagna R, et al. Endovascular repair versus open repair in the treatment of ruptured aortic aneurysms: a systematic review. Minerva Chir. 2019 Dec;74(6):472-80. http://www.ncbi.nlm.nih.gov/pubmed/29806754?tool=bestpractice.com EVAR ასევე მცირდება მუცლის აორტის ანევრიზმით გამოწვეულ სიკვდილობაც(მაგრამ არა გადარჩენადობა ხანგრძლივ პერსპექტივაში) იმ პაციენტებში, რომელთაც დიდი ანევრიზმა აქვთ (≥5.5 სმ) და ვერ უტარდებათ ღია წესით ოპერაცია.[140]Greenhalgh RM, Brown LC, Powell JT, et al; United Kingdom EVAR Trial Investigators. Endovascular repair of aortic aneurysm in patients physically ineligible for open repair. N Engl J Med. 2010 May 20;362(20):1872-80. http://www.ncbi.nlm.nih.gov/pubmed/20382982?tool=bestpractice.com
ოპერაციის შემდგომ, დიდი ზომის ანევრიზმები დაკავშირებულია უფრო ცუდ გრძელვადიან გადარჩენადობასთან, ვიდრე მცირე ზომის ანევრიზმები (ჯამური საფრთხის თანაფარდობა 1.14 ყოველ 1-სმ დიამეტრზე, 95% სარწმუნოობის ინტერვალი 1.09 - 1.18; 12.0- 91.2-თვიანი შემდგომი მეთვალყურეობა).[141]Khashram M, Hider PN, Williman JA, et al. Does the diameter of abdominal aortic aneurysm influence late survival following abdominal aortic aneurysm repair? A systematic review and meta-analysis. Vascular. 2016 Dec;24(6):658-67. http://www.ncbi.nlm.nih.gov/pubmed/27189809?tool=bestpractice.com ეს კავშირი უფრო გამოხატულია EVAR-ის შემთხვევაში ვიდრე ღია წესით შესრულების დროს.
FEVAR წარმოადგენს ღია მიდგომის ალტერნატივას თირკმლის გვერდითა ან ზედა მუცლის აორტის ანევრიზმის შეკეთებისათვის, როცა მოკლე ან დარღვეული კისერი გამორიცხავს ჩვეულებრივ მიდგომას.
პერიოპერაციული კარდიოვასკულარული რისკის შემცირება
მკურნალობა, რომელიც რეკომენდებულია <strong>ყველა</strong> პაციენტისთვის შერჩეულ ჯგუფში
ცვლადი გულსისხლძარღვთა რისკფაქტორების კონტროლი პრეოპერაციულად აუმჯობესებს ჩარევის შემდგომ გადარჩენის სიხშირეს.[190]Khashram M, Williman JA, Hider PN, et al. Management of modifiable vascular risk factors improves late survival following abdominal aortic aneurysm repair: a systematic review and meta-analysis. Ann Vasc Surg. 2017 Feb;39:301-11. http://www.ncbi.nlm.nih.gov/pubmed/27666804?tool=bestpractice.com
პაციენტებს უნდა მიეცეთ რეკომენდაცია მოწევის შეწყვეტასთან დაკავშირებით და უნდა შესთავაზონ, საჭიროების შემთხვევაში, მედიკამენტური მკურნალობა.[1]Dehlin JM, Upchurch GR. Management of abdominal aortic aneurysms. Curr Treat Options Cardiovasc Med. 2005 Jun;7(2):119-30.
http://www.ncbi.nlm.nih.gov/pubmed/15935120?tool=bestpractice.com
[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482.
https://www.doi.org/10.1161/CIR.0000000000001106
http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com
[13]Zankl AR, Schumacher H, Krumsdorf U, et al. Pathology, natural history and treatment of abdominal aortic aneurysms. Clin Res Cardiol. 2007 Mar;96(3):140-51.
http://www.ncbi.nlm.nih.gov/pubmed/17180573?tool=bestpractice.com
[15]Singh K, Bønaa H, Jacobsen BK, et al. Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study: the Tromsø Study. Am J Epidemiol. 2001 Aug 1;154(3):236-44.
https://academic.oup.com/aje/article/154/3/236/125840
http://www.ncbi.nlm.nih.gov/pubmed/11479188?tool=bestpractice.com
[23]Lederle FA, Johnson GR, Wilson SE, et al; Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Prevalence and associations of abdominal aortic aneurysm detected through screening. Ann Intern Med. 1997 Mar 15;126(6):441-9.
http://www.ncbi.nlm.nih.gov/pubmed/9072929?tool=bestpractice.com
[24]Wilmink TB, Quick CR, Day NE. The association between cigarette smoking and abdominal aortic aneurysms. J Vasc Surg. 1999 Dec;30(6):1099-105.
http://www.ncbi.nlm.nih.gov/pubmed/10587395?tool=bestpractice.com
[131]Hartmann-Boyce J, Chepkin SC, Ye W, et al. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst Rev. 2018 May 31;5:CD000146.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000146.pub5/full
http://www.ncbi.nlm.nih.gov/pubmed/29852054?tool=bestpractice.com
[132]Rigotti NA, Clair C, Munafò MR, et al. Interventions for smoking cessation in hospitalised patients. Cochrane Database Syst Rev. 2012 May 16;(5):CD001837.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001837.pub3/full
http://www.ncbi.nlm.nih.gov/pubmed/22592676?tool=bestpractice.com
[133]Howes S, Hartmann-Boyce J, Livingstone-Banks J, et al. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2020 Apr 22;(4):CD000031.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000031.pub5/full
http://www.ncbi.nlm.nih.gov/pubmed/32319681?tool=bestpractice.com
[ ![]() ]
What are the effects of adding bupropion or fluoxetine to other treatments compared with using other treatments alone for people trying to quit smoking?/cca.html?targetUrl=https://www.cochranelibrary.com/cca/doi/10.1002/cca.4337/fullსწორი პასუხის ჩვენება
]
What are the effects of adding bupropion or fluoxetine to other treatments compared with using other treatments alone for people trying to quit smoking?/cca.html?targetUrl=https://www.cochranelibrary.com/cca/doi/10.1002/cca.4337/fullსწორი პასუხის ჩვენება
წინასაოპერაციო ვარჯიშმა ფიზიკური დატვირთვით დააქვეითა პოსტოპერაციული კარდიალური გართულებები მცირე რანდომიზებული კონტროლირებადი კვლევების მიხედვით.პაციენტებში,რომლებმაც გადაიტანეს ღია ან ენდოვასკულარული AAA პლასტიკა, თუმცა კოხრეინის მიმოხილვამ და ოპერაციამდე პრეჰაბილიტაციის (სავარჯიშო ტრენინგის) ცალკეული სისტემატური მიმოხილვამ არ აჩვენა რაიმე შედეგის სარგებელი.[191]Barakat HM, Shahin Y, Khan JA, et al. Preoperative supervised exercise improves outcomes after elective abdominal aortic aneurysm repair: a randomized controlled trial. Ann Surg. 2016 Jul;264(1):47-53. http://www.ncbi.nlm.nih.gov/pubmed/26756766?tool=bestpractice.com [192]Fenton C, Tan AR, Abaraogu UO, et al. Prehabilitation exercise therapy before elective abdominal aortic aneurysm repair. Cochrane Database Syst Rev. 2021 Jul 8;7(7):CD013662. https://www.doi.org/10.1002/14651858.CD013662.pub2 http://www.ncbi.nlm.nih.gov/pubmed/34236703?tool=bestpractice.com [193]Bonner RJ, Wallace T, Jones AD, et al. The content of pre-habilitative interventions for patients undergoing repair of abdominal aortic aneurysms and their effect on post-operative outcomes: a systematic review. Eur J Vasc Endovasc Surg. 2021 May;61(5):756-65. https://www.doi.org/10.1016/j.ejvs.2021.01.043 http://www.ncbi.nlm.nih.gov/pubmed/33678532?tool=bestpractice.com მიუხედავად იმისა, რომ წინასაოპერაციო ვარჯიში შეიძლება სასარგებლო იყოს პაციენტებისთვის, რომლებიც გადიან AAA-ს პლასტიკას, საჭიროა შემდგომი გამოკვლევა RCT-ებით, სანამ ის უფრო ფართოდ იქნება რეკომენდებული.[194]Wee IJY, Choong AMTL. A systematic review of the impact of preoperative exercise for patients with abdominal aortic aneurysm. J Vasc Surg. 2020 Jun;71(6):2123-31.e1. https://www.doi.org/10.1016/j.jvs.2018.09.039 http://www.ncbi.nlm.nih.gov/pubmed/30606665?tool=bestpractice.com
პერიოპერაციული სტატინების გამოყენება ანელებს ანევრიზმის ზრდას, ამცირებს რღვევის რისკს და ამცირებს სიკვდილიანობას AAA-ს პლასტიკის ან გახეთქილი AAA-სგან.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com სტატინები უნდა დაინიშნოს ქირურგიულ ჩარევამდე სულ მცირე 1 თვით ადრე, რათა შემცირდეს გულსისხლძარღვთა მიზეზით სიკვდილობა. სტატინები გრძელდება განუსაზღვრელი ვადით.[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com [136]Risum Ø, Sandven I, Sundhagen JO, et al. Editor's choice - effect of statins on total mortality in abdominal aortic aneurysm repair: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2021 Jan;61(1):114-20. https://www.doi.org/10.1016/j.ejvs.2020.08.007 http://www.ncbi.nlm.nih.gov/pubmed/32928667?tool=bestpractice.com
პაციენტებს AAA-ით აქვთ მაღალი რისკი გულ-სისხლძარღვთა დაავადებების სერიოზული გართულებების მხრივ. არსებობს შეზღუდული მტკიცებულება, მაგრამ რაიმე უკუჩვენების არარსებობის შემთხვევაში, AAA-ს მქონე პაციენტებმა უნდა მიიღონ ერთჯერადი ანტითრომბოციტული თერაპია (ასპირინი ან კლოპიდოგრელი).[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [137]Aboyans V, Bauersachs R, Mazzolai L, et al. Antithrombotic therapies in aortic and peripheral arterial diseases in 2021: a consensus document from the ESC working group on aorta and peripheral vascular diseases, the ESC working group on thrombosis, and the ESC working group on cardiovascular pharmacotherapy. Eur Heart J. 2021 Oct 14;42(39):4013-24. https://www.doi.org/10.1093/eurheartj/ehab390 http://www.ncbi.nlm.nih.gov/pubmed/34279602?tool=bestpractice.com დააკვირდეთ პაციენტებს პერიოპერაციულ პერიოდში[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
ჰიპერტენზია უნდა გაკონტროლდეს გულსისხლძარღვთა ავადობის შესამცირებლად.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
პერიოპერაციული ანტიბიოტიკოთერაპია
მკურნალობა, რომელიც რეკომენდებულია <strong>ყველა</strong> პაციენტისთვის შერჩეულ ჯგუფში
ჩაუტარდა პერიოპერაციული ანტიბიოტიკოთერაპია. ფართო სპექტრის ანტიბიოტიკებით პროფილაქტიკა აუცილებელია, ადგილობრივი პროტოკოლის თანახმად.
ინფექციურ-ანთებითი პროცესების მკურნალობა.
დამატებითი მკურნალობა, რომელიც რეკომენდებულია <strong>ზოგიერთი</strong> პაციენტისთვის შერჩეული ჯგუფიდან
უნდა განიხილებოდეს ინფექციური ან ანთებითი ეტიოლოგია.
თუ პაციენტს აქვს საეჭვო ინფექციური ანევრიზმა, ადრეული დიაგნოსტიკა, დროული მკურნალობა ანტიბიოტიკებით და სასწრაფო ქირურგიული ჩარევა აუცილებელია შედეგების გასაუმჯობესებლად.[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com ამ პაციენტებში გადაუდებელი ქირურგიული ჩარევის დროს ხშირად საჭირო ხდება ფართო სანაცია. არსებობს მეორადი ინფექციური გართულებების მაღალი რისკი და შეიძლება საჭირო გახდეს შემდგომი ოპერაცია ახალი ინფექციური დაზიანებისთვის. ინტრაოპერაციული კულტურები უნდა იქნას მიღებული შემდგომი ანტიბიოტიკოთერაპიის სწორად წარმართვისთვის; თუმცა, ემპირიული ანტიბიოტიკები ხშირად ინიშნება, რადგან პერიფერიული სისხლის კულტურები და ქირურგიული ნიმუშების კულტურები ნეგატიურია პაციენტთა დიდ ნაწილში.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com შესაძლოა ნაჩვენები იყოს ხანგრძლივი ანტიბიოტიკოთერაპია (4-6 კვირიდან სიცოცხლის ხანგრძლივ პერიოდში) სპეციფიკური პათოგენის, ოპერაციული პლასტიკის ტიპისა და პაციენტის იმუნოლოგიური მდგომარეობის მიხედვით.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
ანთებითი აორტიტის დროს (გამოწვეული, მაგალითად, ტაკაიასუს არტერიტით ან გიგანტურუჯრედოვანი არტერიტით) მკურნალობა ხდება კორტიკოსტეროიდების მაღალი დოზით და ქირურგიული ჩარევით.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [200]Ben Jmaà H, Karray R, Jmal H, et al. Surgical and endoluminal management of the inflammatory aortitis: a Tunisian center experience [in French]. J Med Vasc. 2017 Jul;42(4):213-20. http://www.ncbi.nlm.nih.gov/pubmed/28705339?tool=bestpractice.com
ენდოვასკულური ჩარევის შემდგომი გაჟონვა, რომელსაც ესაჭიროება მკურნალობა
მაკორექტირებელი პროცედურები
შინაგანი გაჟონვა (endoleak) არის, როდესაც სისხლის ნაკადი მუდმივად გადის გრაფტის გარეთ, ანევრიზმის პარკში.[201]Schurink GW, Aarts NJ, vanBockel JH. Endoleak after stent-graft treatment of abdominal aortic aneurysm: a meta-analysis of clinical studies. Br J Surg. 1999 May;86(5):581-7. http://www.ncbi.nlm.nih.gov/pubmed/10361173?tool=bestpractice.com [202]Veith FJ, Baum RA, Ohki T, et al. Nature and significance of endoleaks and endotension: summary of opinions expressed at an international conference. J Vasc Surg. 2002 May;35(5):1029-35. http://www.ncbi.nlm.nih.gov/pubmed/12021724?tool=bestpractice.com არ წარმოადგენს ღია წესით მკურნალობის გართულებას.
პოსტოპერაციული მეთვალყურეობით შესაძლებელია გამოხატული გაჟონვების და ანევრიზმის პარკის გადიდების დაფიქსირება. ენდოვასკულური მკურნალობის (EVAR) შემდგომ ენდოგაჟონვის რისკი არის 24%.[201]Schurink GW, Aarts NJ, vanBockel JH. Endoleak after stent-graft treatment of abdominal aortic aneurysm: a meta-analysis of clinical studies. Br J Surg. 1999 May;86(5):581-7. http://www.ncbi.nlm.nih.gov/pubmed/10361173?tool=bestpractice.com არსებობს 5 ტიპის შინაგანი გაჟონვა[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com
მიმაგრების ადგილებიდან (ტიპი Iა ენდო-პროთეზის ან თეძოს ოკლუდერის პროქსიმულ ბოლოში; ტიპი Iბ დისტალურ ბოლოში) გაჟონვა, ჩვეულებრივ, დაუყოვნებლივ ხდება, მაგრამ შესაძლებელია იყოს მოგვიანებითაც.[Figure caption and citation for the preceding image starts]: I ტიპის შინაგანი გაჟონვა მარცხენა ბარძაყის ანასტომოზის დისტალურად (შინაგანი გაჟონვა შემოფარგლულია)მიჩიგანის უნივერსიტეტი, კერძოდ სისხლძარღვთა ქირურგიისა და რადიოლოგიის განყოფილების ექ. აპჩერჩის შემთხვევები [Citation ends]. პროცედურის დამთავრების წინ უნდა ვეცადოთ ავიცილოთ თავიდან I ტიპის ენდოგაჟონვა, (მაგალითად,პროქსიმალური ზონის ბალონირება, პროქსიმალური მანჟეტის დადება, ენდოსტეპლერი).[203]van Schaik TG, Meekel JP, Hoksbergen AWJ, et al. Systematic review of embolization of type I endoleaks using liquid embolic agents. J Vasc Surg. 2021 Sep;74(3):1024-32.
https://www.doi.org/10.1016/j.jvs.2021.03.061
http://www.ncbi.nlm.nih.gov/pubmed/33940072?tool=bestpractice.com
თუ IA ტიპის გაჟონვა პერსისტირებს, შეიძლება საჭირო გახდეს ღია მეთოდზე გადასვლა.[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2.
https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com
[204]Perini P, Bianchini Massoni C, Mariani E, et al. Systematic review and meta-analysis of the outcome of different treatments for type 1a endoleak after EVAR. Ann Vasc Surg. 2019 Oct;60:435-46.e1.
http://www.ncbi.nlm.nih.gov/pubmed/31200054?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: გასაფართოვებელი სტენტის იმპლანტის ჩაყენება ხდება იგივე I ტიპის შინაგანი გაჟონვის (შემოფარგლული) გამო.მიჩიგანის უნივერსიტეტი, კერძოდ სისხლძარღვთა ქირურგიისა და რადიოლოგიის განყოფილების ექ. აპჩერჩის შემთხვევები [Citation ends].
პროცედურის დამთავრების წინ უნდა ვეცადოთ ავიცილოთ თავიდან I ტიპის ენდოგაჟონვა, (მაგალითად,პროქსიმალური ზონის ბალონირება, პროქსიმალური მანჟეტის დადება, ენდოსტეპლერი).[203]van Schaik TG, Meekel JP, Hoksbergen AWJ, et al. Systematic review of embolization of type I endoleaks using liquid embolic agents. J Vasc Surg. 2021 Sep;74(3):1024-32.
https://www.doi.org/10.1016/j.jvs.2021.03.061
http://www.ncbi.nlm.nih.gov/pubmed/33940072?tool=bestpractice.com
თუ IA ტიპის გაჟონვა პერსისტირებს, შეიძლება საჭირო გახდეს ღია მეთოდზე გადასვლა.[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2.
https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com
[204]Perini P, Bianchini Massoni C, Mariani E, et al. Systematic review and meta-analysis of the outcome of different treatments for type 1a endoleak after EVAR. Ann Vasc Surg. 2019 Oct;60:435-46.e1.
http://www.ncbi.nlm.nih.gov/pubmed/31200054?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: გასაფართოვებელი სტენტის იმპლანტის ჩაყენება ხდება იგივე I ტიპის შინაგანი გაჟონვის (შემოფარგლული) გამო.მიჩიგანის უნივერსიტეტი, კერძოდ სისხლძარღვთა ქირურგიისა და რადიოლოგიის განყოფილების ექ. აპჩერჩის შემთხვევები [Citation ends].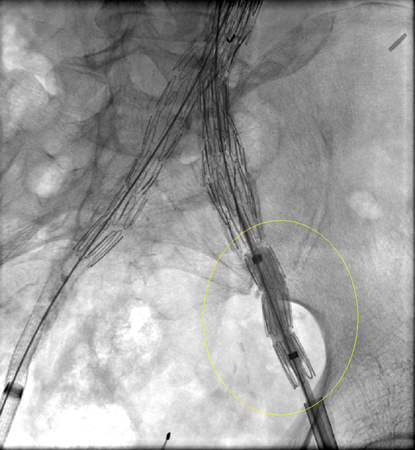 [Figure caption and citation for the preceding image starts]: I ტიპის შინაგანი გაჟონვის პრობლემის გადაჭრა ხდება დამატებითი იმპლანტის (გაგრძელების) დამატებით.მიჩიგანის უნივერსიტეტი, კერძოდ სისხლძარღვთა ქირურგიისა და რადიოლოგიის განყოფილების ექ. აპჩერჩის შემთხვევები [Citation ends].
[Figure caption and citation for the preceding image starts]: I ტიპის შინაგანი გაჟონვის პრობლემის გადაჭრა ხდება დამატებითი იმპლანტის (გაგრძელების) დამატებით.მიჩიგანის უნივერსიტეტი, კერძოდ სისხლძარღვთა ქირურგიისა და რადიოლოგიის განყოფილების ექ. აპჩერჩის შემთხვევები [Citation ends].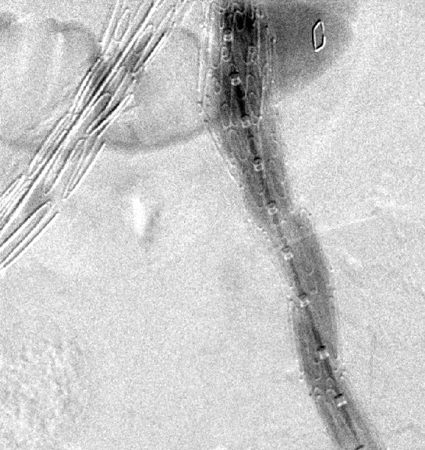
ტიპი II: პატენტის გაჟონვა.[Figure caption and citation for the preceding image starts]: II ტიპის შინაგანი გაჟონვის (შემოფარგლული) აღმოჩენა ხდება ოპერაციის შემდგმი საკონტროლო კომპიუტერული ტომოგრაფიითმიჩიგანის უნივერსიტეტი, კერძოდ სისხლძარღვთა ქირურგიისა და რადიოლოგიის განყოფილების ექ. აპჩერჩის შემთხვევები [Citation ends].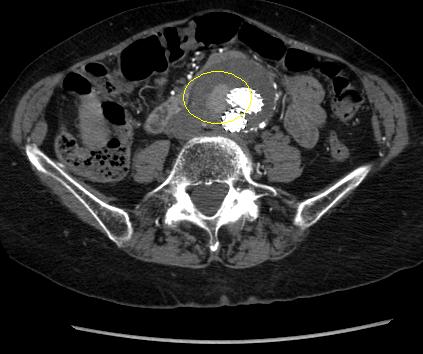 შესაძლებელი შეჩერდეს სპონტანურად, თუმცა ხანგრძლივა ჟონვამ შეიძლება გამოიწვიოს ანევრიზმის პარკის ზრდა.[205]Higashiura W, Greenberg RK, Katz E, et al. Predictive factors, morphologic effects, and proposed treatment paradigm for type II endoleaks after repair of infrarenal abdominal aortic aneurysms. J Vasc Interv Radiol. 2007 Aug;18(8):975-81.
http://www.ncbi.nlm.nih.gov/pubmed/17675614?tool=bestpractice.com
თუ EVAR-ის შემდეგ 1 თვეში, კონტრასტული კტ კვლევით,II ტიპის შინაგანი გაჟონვა ან სხვა პრობლემა აღინიშნება, რეკომენდებულია ოპერაციიდან 6 თვეში კვლევის განმეორებით ჩატარება.[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2.
https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com
IIტიპის ენდოგაჟონვის დაახლოებით 50% დიაგნოზირებულია 30-დღიან დაკვირვებამდე; 40% 30 დღის შემდეგ და 8% დიაგნოზირებულია მეთვალყურეობის 12 თვის შემდეგ.[206]Charisis N, Bouris V, Conway AM, et al. A systematic review and pooled meta-analysis on the incidence and temporal occurrence of type II endoleak following an abdominal aortic aneurysm repair. Ann Vasc Surg. 2021 Aug;75:406-19.
http://www.ncbi.nlm.nih.gov/pubmed/33549794?tool=bestpractice.com
მკურნალობა რჩება საკამათო და მოწოდებულია 6-12 თვის განმავლობაში უცვლელი ზომის შემთხვევაში, ან თუ ანევრიზმის პარკის ზომა იმატებს ისე, რომ პროქსიმალური და/ან დისტალური ზონები შეიძლება დაირღვეს.[207]Mansueto G, Cenzi D, Scuro A, et al. Treatment of type II endoleak with a transcatheter transcaval approach: results at 1-year follow-up. J Vasc Surg. 2007 Jun;45(6):1120-7.
http://www.ncbi.nlm.nih.gov/pubmed/17543674?tool=bestpractice.com
[208]Baum RA, Stavropoulos SW, Fairman RM, et al. Endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2003 Sep;14(9 Pt 1):1111-7.
http://www.ncbi.nlm.nih.gov/pubmed/14514802?tool=bestpractice.com
[209]Van Marrewijk CJ, Fransen G, Laheij RJ, et al. Is a type II endoleak after EVAR a harbinger of risk? Causes and outcome of open conversion and aneurysm rupture during follow-up. Eur J Vasc Endovasc Surg. 2004 Feb;27(2):128-37.
http://www.ncbi.nlm.nih.gov/pubmed/14718893?tool=bestpractice.com
[210]Harris PL, Vallabhaneni SR, Desgranges P, et al. Incidence and risk factors of late rupture, conversion, and death after endovascular repair of infrarenal aortic aneurysms: the EUROSTAR experience. J Vasc Surg. 2000 Oct;32(4):739-49.
http://www.ncbi.nlm.nih.gov/pubmed/11013038?tool=bestpractice.com
[211]Ultee KHJ, Büttner S, Huurman R, et al. Editor's choice - systematic review and meta-analysis of the outcome of treatment for type II endoleak following endovascular aneurysm repair. Eur J Vasc Endovasc Surg. 2018 Dec;56(6):794-807.
https://www.doi.org/10.1016/j.ejvs.2018.06.009
http://www.ncbi.nlm.nih.gov/pubmed/30104089?tool=bestpractice.com
[212]Smith T, Quencer KB. Best practice guidelines: imaging surveillance after endovascular aneurysm repair. AJR Am J Roentgenol. 2020 May;214(5):1165-74.
https://www.doi.org/10.2214/AJR.19.22197
http://www.ncbi.nlm.nih.gov/pubmed/32130043?tool=bestpractice.com
მკურნალობის უპირატესი მეთოდია ტრანსარტერიულად სპირალით ემბოლიზაცია, თუმცა ასევე აღრიცხულია კოლატერალური სისხლძარღვების ლაპარასკოპიული ლიგირების, ანევრიზმის პარკის პირდაპირი პერკუტანეული ტრანსლუმბალური პუნქციის, ტრანსლუმბალური ემბოლიზაციის და ტრანსკათეტერული ტრანსკავალური ემბოლიზაციის მეთოდებიც.[202]Veith FJ, Baum RA, Ohki T, et al. Nature and significance of endoleaks and endotension: summary of opinions expressed at an international conference. J Vasc Surg. 2002 May;35(5):1029-35.
http://www.ncbi.nlm.nih.gov/pubmed/12021724?tool=bestpractice.com
[207]Mansueto G, Cenzi D, Scuro A, et al. Treatment of type II endoleak with a transcatheter transcaval approach: results at 1-year follow-up. J Vasc Surg. 2007 Jun;45(6):1120-7.
http://www.ncbi.nlm.nih.gov/pubmed/17543674?tool=bestpractice.com
[208]Baum RA, Stavropoulos SW, Fairman RM, et al. Endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2003 Sep;14(9 Pt 1):1111-7.
http://www.ncbi.nlm.nih.gov/pubmed/14514802?tool=bestpractice.com
[209]Van Marrewijk CJ, Fransen G, Laheij RJ, et al. Is a type II endoleak after EVAR a harbinger of risk? Causes and outcome of open conversion and aneurysm rupture during follow-up. Eur J Vasc Endovasc Surg. 2004 Feb;27(2):128-37.
http://www.ncbi.nlm.nih.gov/pubmed/14718893?tool=bestpractice.com
[213]Steinmetz E, Rubin BG, Sanchez LA, et al. Type II endoleak after endovascular abdominal aortic aneurysm repair: a conservative approach with selective intervention is safe and cost-effective. J Vasc Surg. 2004 Feb;39(2):306-13.
http://www.ncbi.nlm.nih.gov/pubmed/14743129?tool=bestpractice.com
[214]Baum RA, Cope C, Fairman, et al. Translumbar embolization of type 2 endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2001 Jan;12(1):111-6.
http://www.ncbi.nlm.nih.gov/pubmed/11200344?tool=bestpractice.com
[215]Baum RA, Carpenter JP, Golden MA, et al. Treatment of type 2 endoleaks after endovascular repair of abdominal aortic aneurysms: comparison of transarterial and translumbar techniques. J Vasc Surg. 2002 Jan;35(1):23-9.
http://www.ncbi.nlm.nih.gov/pubmed/11802129?tool=bestpractice.com
[216]Schmid R, Gurke L, Aschwanden M, et al. CT-guided percutaneous embolization of a lumbar artery maintaining a type II endoleak. J Endovasc Ther. 2002 Apr;9(2):198-202.
http://www.ncbi.nlm.nih.gov/pubmed/12010100?tool=bestpractice.com
[217]Chin KM, Lee SQW, Lee HJ, et al. Preservation of stent graft after iatrogenic type III endoleak during open transperitoneal surgical intervention for complicated type II endoleak. Ann Vasc Surg. 2020 Jan;62:496.e1-496.e7.
http://www.ncbi.nlm.nih.gov/pubmed/31394250?tool=bestpractice.com
[218]Li Q, Hou P. Sac embolization and side branch embolization for preventing type II endoleaks after endovascular aneurysm repair: a meta-analysis. J Endovasc Ther. 2020 Feb;27(1):109-16.
https://www.doi.org/10.1177/1526602819878411
http://www.ncbi.nlm.nih.gov/pubmed/31566053?tool=bestpractice.com
[219]Akmal MM, Pabittei DR, Prapassaro T, et al. A systematic review of the current status of interventions for type II endoleak after EVAR for abdominal aortic aneurysms. Int J Surg. 2021 Nov;95:106138.
https://www.doi.org/10.1016/j.ijsu.2021.106138
http://www.ncbi.nlm.nih.gov/pubmed/34637951?tool=bestpractice.com
[220]Yu HYH, Lindström D, Wanhainen A, et al. Systematic review and meta-analysis of prophylactic aortic side branch embolization to prevent type II endoleaks. J Vasc Surg. 2020 Nov;72(5):1783-1792.e1.
https://www.doi.org/10.1016/j.jvs.2020.05.020
http://www.ncbi.nlm.nih.gov/pubmed/32442608?tool=bestpractice.com
[221]Zhang X, Ji L, Chen MY, et al. Transarterial embolization versus translumber embolization for type Ⅱ endoleak after endovascular abdominal aortic aneurysm repair: a meta-analysis. Chin Med Sci J. 2020 Jun 30;35(2):135-41.
https://www.doi.org/10.24920/003618
http://www.ncbi.nlm.nih.gov/pubmed/32684233?tool=bestpractice.com
შესაძლებელი შეჩერდეს სპონტანურად, თუმცა ხანგრძლივა ჟონვამ შეიძლება გამოიწვიოს ანევრიზმის პარკის ზრდა.[205]Higashiura W, Greenberg RK, Katz E, et al. Predictive factors, morphologic effects, and proposed treatment paradigm for type II endoleaks after repair of infrarenal abdominal aortic aneurysms. J Vasc Interv Radiol. 2007 Aug;18(8):975-81.
http://www.ncbi.nlm.nih.gov/pubmed/17675614?tool=bestpractice.com
თუ EVAR-ის შემდეგ 1 თვეში, კონტრასტული კტ კვლევით,II ტიპის შინაგანი გაჟონვა ან სხვა პრობლემა აღინიშნება, რეკომენდებულია ოპერაციიდან 6 თვეში კვლევის განმეორებით ჩატარება.[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2.
https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com
IIტიპის ენდოგაჟონვის დაახლოებით 50% დიაგნოზირებულია 30-დღიან დაკვირვებამდე; 40% 30 დღის შემდეგ და 8% დიაგნოზირებულია მეთვალყურეობის 12 თვის შემდეგ.[206]Charisis N, Bouris V, Conway AM, et al. A systematic review and pooled meta-analysis on the incidence and temporal occurrence of type II endoleak following an abdominal aortic aneurysm repair. Ann Vasc Surg. 2021 Aug;75:406-19.
http://www.ncbi.nlm.nih.gov/pubmed/33549794?tool=bestpractice.com
მკურნალობა რჩება საკამათო და მოწოდებულია 6-12 თვის განმავლობაში უცვლელი ზომის შემთხვევაში, ან თუ ანევრიზმის პარკის ზომა იმატებს ისე, რომ პროქსიმალური და/ან დისტალური ზონები შეიძლება დაირღვეს.[207]Mansueto G, Cenzi D, Scuro A, et al. Treatment of type II endoleak with a transcatheter transcaval approach: results at 1-year follow-up. J Vasc Surg. 2007 Jun;45(6):1120-7.
http://www.ncbi.nlm.nih.gov/pubmed/17543674?tool=bestpractice.com
[208]Baum RA, Stavropoulos SW, Fairman RM, et al. Endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2003 Sep;14(9 Pt 1):1111-7.
http://www.ncbi.nlm.nih.gov/pubmed/14514802?tool=bestpractice.com
[209]Van Marrewijk CJ, Fransen G, Laheij RJ, et al. Is a type II endoleak after EVAR a harbinger of risk? Causes and outcome of open conversion and aneurysm rupture during follow-up. Eur J Vasc Endovasc Surg. 2004 Feb;27(2):128-37.
http://www.ncbi.nlm.nih.gov/pubmed/14718893?tool=bestpractice.com
[210]Harris PL, Vallabhaneni SR, Desgranges P, et al. Incidence and risk factors of late rupture, conversion, and death after endovascular repair of infrarenal aortic aneurysms: the EUROSTAR experience. J Vasc Surg. 2000 Oct;32(4):739-49.
http://www.ncbi.nlm.nih.gov/pubmed/11013038?tool=bestpractice.com
[211]Ultee KHJ, Büttner S, Huurman R, et al. Editor's choice - systematic review and meta-analysis of the outcome of treatment for type II endoleak following endovascular aneurysm repair. Eur J Vasc Endovasc Surg. 2018 Dec;56(6):794-807.
https://www.doi.org/10.1016/j.ejvs.2018.06.009
http://www.ncbi.nlm.nih.gov/pubmed/30104089?tool=bestpractice.com
[212]Smith T, Quencer KB. Best practice guidelines: imaging surveillance after endovascular aneurysm repair. AJR Am J Roentgenol. 2020 May;214(5):1165-74.
https://www.doi.org/10.2214/AJR.19.22197
http://www.ncbi.nlm.nih.gov/pubmed/32130043?tool=bestpractice.com
მკურნალობის უპირატესი მეთოდია ტრანსარტერიულად სპირალით ემბოლიზაცია, თუმცა ასევე აღრიცხულია კოლატერალური სისხლძარღვების ლაპარასკოპიული ლიგირების, ანევრიზმის პარკის პირდაპირი პერკუტანეული ტრანსლუმბალური პუნქციის, ტრანსლუმბალური ემბოლიზაციის და ტრანსკათეტერული ტრანსკავალური ემბოლიზაციის მეთოდებიც.[202]Veith FJ, Baum RA, Ohki T, et al. Nature and significance of endoleaks and endotension: summary of opinions expressed at an international conference. J Vasc Surg. 2002 May;35(5):1029-35.
http://www.ncbi.nlm.nih.gov/pubmed/12021724?tool=bestpractice.com
[207]Mansueto G, Cenzi D, Scuro A, et al. Treatment of type II endoleak with a transcatheter transcaval approach: results at 1-year follow-up. J Vasc Surg. 2007 Jun;45(6):1120-7.
http://www.ncbi.nlm.nih.gov/pubmed/17543674?tool=bestpractice.com
[208]Baum RA, Stavropoulos SW, Fairman RM, et al. Endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2003 Sep;14(9 Pt 1):1111-7.
http://www.ncbi.nlm.nih.gov/pubmed/14514802?tool=bestpractice.com
[209]Van Marrewijk CJ, Fransen G, Laheij RJ, et al. Is a type II endoleak after EVAR a harbinger of risk? Causes and outcome of open conversion and aneurysm rupture during follow-up. Eur J Vasc Endovasc Surg. 2004 Feb;27(2):128-37.
http://www.ncbi.nlm.nih.gov/pubmed/14718893?tool=bestpractice.com
[213]Steinmetz E, Rubin BG, Sanchez LA, et al. Type II endoleak after endovascular abdominal aortic aneurysm repair: a conservative approach with selective intervention is safe and cost-effective. J Vasc Surg. 2004 Feb;39(2):306-13.
http://www.ncbi.nlm.nih.gov/pubmed/14743129?tool=bestpractice.com
[214]Baum RA, Cope C, Fairman, et al. Translumbar embolization of type 2 endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2001 Jan;12(1):111-6.
http://www.ncbi.nlm.nih.gov/pubmed/11200344?tool=bestpractice.com
[215]Baum RA, Carpenter JP, Golden MA, et al. Treatment of type 2 endoleaks after endovascular repair of abdominal aortic aneurysms: comparison of transarterial and translumbar techniques. J Vasc Surg. 2002 Jan;35(1):23-9.
http://www.ncbi.nlm.nih.gov/pubmed/11802129?tool=bestpractice.com
[216]Schmid R, Gurke L, Aschwanden M, et al. CT-guided percutaneous embolization of a lumbar artery maintaining a type II endoleak. J Endovasc Ther. 2002 Apr;9(2):198-202.
http://www.ncbi.nlm.nih.gov/pubmed/12010100?tool=bestpractice.com
[217]Chin KM, Lee SQW, Lee HJ, et al. Preservation of stent graft after iatrogenic type III endoleak during open transperitoneal surgical intervention for complicated type II endoleak. Ann Vasc Surg. 2020 Jan;62:496.e1-496.e7.
http://www.ncbi.nlm.nih.gov/pubmed/31394250?tool=bestpractice.com
[218]Li Q, Hou P. Sac embolization and side branch embolization for preventing type II endoleaks after endovascular aneurysm repair: a meta-analysis. J Endovasc Ther. 2020 Feb;27(1):109-16.
https://www.doi.org/10.1177/1526602819878411
http://www.ncbi.nlm.nih.gov/pubmed/31566053?tool=bestpractice.com
[219]Akmal MM, Pabittei DR, Prapassaro T, et al. A systematic review of the current status of interventions for type II endoleak after EVAR for abdominal aortic aneurysms. Int J Surg. 2021 Nov;95:106138.
https://www.doi.org/10.1016/j.ijsu.2021.106138
http://www.ncbi.nlm.nih.gov/pubmed/34637951?tool=bestpractice.com
[220]Yu HYH, Lindström D, Wanhainen A, et al. Systematic review and meta-analysis of prophylactic aortic side branch embolization to prevent type II endoleaks. J Vasc Surg. 2020 Nov;72(5):1783-1792.e1.
https://www.doi.org/10.1016/j.jvs.2020.05.020
http://www.ncbi.nlm.nih.gov/pubmed/32442608?tool=bestpractice.com
[221]Zhang X, Ji L, Chen MY, et al. Transarterial embolization versus translumber embolization for type Ⅱ endoleak after endovascular abdominal aortic aneurysm repair: a meta-analysis. Chin Med Sci J. 2020 Jun 30;35(2):135-41.
https://www.doi.org/10.24920/003618
http://www.ncbi.nlm.nih.gov/pubmed/32684233?tool=bestpractice.com
III ტიპი: გრაფტის დეფექტი ქსოვილის რღვევითი გაჟონვით, ნამყენის გათიშვით ან ქსოვილის დაშლით.[201]Schurink GW, Aarts NJ, vanBockel JH. Endoleak after stent-graft treatment of abdominal aortic aneurysm: a meta-analysis of clinical studies. Br J Surg. 1999 May;86(5):581-7. http://www.ncbi.nlm.nih.gov/pubmed/10361173?tool=bestpractice.com [202]Veith FJ, Baum RA, Ohki T, et al. Nature and significance of endoleaks and endotension: summary of opinions expressed at an international conference. J Vasc Surg. 2002 May;35(5):1029-35. http://www.ncbi.nlm.nih.gov/pubmed/12021724?tool=bestpractice.com [222]Kwon J, Dimuzio P, Salvatore D, et al. Incidence of stent graft failure from type IIIB endoleak in contemporary endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2020 Feb;71(2):645-53. https://www.doi.org/10.1016/j.jvs.2019.06.183 http://www.ncbi.nlm.nih.gov/pubmed/31466740?tool=bestpractice.com ჩარევა ნაჩვენებია აღმოჩენისთანავე ენდოვასკულური გაფართოება სტენტის იმპლანტით).[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2. https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com [208]Baum RA, Stavropoulos SW, Fairman RM, et al. Endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2003 Sep;14(9 Pt 1):1111-7. http://www.ncbi.nlm.nih.gov/pubmed/14514802?tool=bestpractice.com [212]Smith T, Quencer KB. Best practice guidelines: imaging surveillance after endovascular aneurysm repair. AJR Am J Roentgenol. 2020 May;214(5):1165-74. https://www.doi.org/10.2214/AJR.19.22197 http://www.ncbi.nlm.nih.gov/pubmed/32130043?tool=bestpractice.com [223]Lowe C, Hansrani V, Madan M, et al. Type IIIb endoleak after elective endovascular aneurysm repair: a systematic review. J Cardiovasc Surg (Torino). 2020 Jun;61(3):308-16. http://www.ncbi.nlm.nih.gov/pubmed/29616524?tool=bestpractice.com
ტიპი IV: გაჟონვა გრაფტის კედლის ფორიანობიდან.[201]Schurink GW, Aarts NJ, vanBockel JH. Endoleak after stent-graft treatment of abdominal aortic aneurysm: a meta-analysis of clinical studies. Br J Surg. 1999 May;86(5):581-7. http://www.ncbi.nlm.nih.gov/pubmed/10361173?tool=bestpractice.com [202]Veith FJ, Baum RA, Ohki T, et al. Nature and significance of endoleaks and endotension: summary of opinions expressed at an international conference. J Vasc Surg. 2002 May;35(5):1029-35. http://www.ncbi.nlm.nih.gov/pubmed/12021724?tool=bestpractice.com ეს გაჟონვა იშვიათია ახალი სტენტების იმპლანტირებისას და თვითგანკურნებადია.[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2. https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com [208]Baum RA, Stavropoulos SW, Fairman RM, et al. Endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2003 Sep;14(9 Pt 1):1111-7. http://www.ncbi.nlm.nih.gov/pubmed/14514802?tool=bestpractice.com
ტიპი V (ენდოტენზია): ენდოტენზია არის გაზრდილი ინტრასაკური წნევა EVAR-ის შემდეგ ვიზუალური ენდოგაჟონვის გარეშე დაგვიანებული კონტრასტული CT სკანირებისას. ნაკლებად გავრცელებულია ახალი თაობის გრაფტებთან.[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2. https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com არ არსებობს შინაგანი წნევის გაზომვის სტანდარტიზებული მეთოდი და რეკომენდებული მკურნალობის შესახებ კონსენსუსი თუ არ აღინიშნება ანევრიზმის გაფართოება; თუმცა, შინაგანი წნევის შესამცირებლად მკურნალობა ანევრიზმის გასკდომის თავიდან აცილების მიზნით რეკომენდებულია პაციენტების გარკვეული ჯგუფისათვის, რომელთაც აღენიშნებათ ანევრიზმის დროში გახანგრძლივებული გაფართოება.[78]Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-77.e2. https://www.jvascsurg.org/article/S0741-5214(17)32369-8/fulltext http://www.ncbi.nlm.nih.gov/pubmed/29268916?tool=bestpractice.com [202]Veith FJ, Baum RA, Ohki T, et al. Nature and significance of endoleaks and endotension: summary of opinions expressed at an international conference. J Vasc Surg. 2002 May;35(5):1029-35. http://www.ncbi.nlm.nih.gov/pubmed/12021724?tool=bestpractice.com [212]Smith T, Quencer KB. Best practice guidelines: imaging surveillance after endovascular aneurysm repair. AJR Am J Roentgenol. 2020 May;214(5):1165-74. https://www.doi.org/10.2214/AJR.19.22197 http://www.ncbi.nlm.nih.gov/pubmed/32130043?tool=bestpractice.com
პერიოპერაციული კარდიოვასკულარული რისკის შემცირება
მკურნალობა, რომელიც რეკომენდებულია <strong>ყველა</strong> პაციენტისთვის შერჩეულ ჯგუფში
ცვლადი გულსისხლძარღვთა რისკფაქტორების კონტროლი პრეოპერაციულად აუმჯობესებს ჩარევის შემდგომ გადარჩენის სიხშირეს.[190]Khashram M, Williman JA, Hider PN, et al. Management of modifiable vascular risk factors improves late survival following abdominal aortic aneurysm repair: a systematic review and meta-analysis. Ann Vasc Surg. 2017 Feb;39:301-11. http://www.ncbi.nlm.nih.gov/pubmed/27666804?tool=bestpractice.com
პაციენტებს უნდა მიეცეთ რეკომენდაცია მოწევის შეწყვეტასთან დაკავშირებით და უნდა შესთავაზონ, საჭიროების შემთხვევაში, მედიკამენტური მკურნალობა.[1]Dehlin JM, Upchurch GR. Management of abdominal aortic aneurysms. Curr Treat Options Cardiovasc Med. 2005 Jun;7(2):119-30.
http://www.ncbi.nlm.nih.gov/pubmed/15935120?tool=bestpractice.com
[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482.
https://www.doi.org/10.1161/CIR.0000000000001106
http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com
[13]Zankl AR, Schumacher H, Krumsdorf U, et al. Pathology, natural history and treatment of abdominal aortic aneurysms. Clin Res Cardiol. 2007 Mar;96(3):140-51.
http://www.ncbi.nlm.nih.gov/pubmed/17180573?tool=bestpractice.com
[15]Singh K, Bønaa H, Jacobsen BK, et al. Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study: the Tromsø Study. Am J Epidemiol. 2001 Aug 1;154(3):236-44.
https://academic.oup.com/aje/article/154/3/236/125840
http://www.ncbi.nlm.nih.gov/pubmed/11479188?tool=bestpractice.com
[23]Lederle FA, Johnson GR, Wilson SE, et al; Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Prevalence and associations of abdominal aortic aneurysm detected through screening. Ann Intern Med. 1997 Mar 15;126(6):441-9.
http://www.ncbi.nlm.nih.gov/pubmed/9072929?tool=bestpractice.com
[24]Wilmink TB, Quick CR, Day NE. The association between cigarette smoking and abdominal aortic aneurysms. J Vasc Surg. 1999 Dec;30(6):1099-105.
http://www.ncbi.nlm.nih.gov/pubmed/10587395?tool=bestpractice.com
[131]Hartmann-Boyce J, Chepkin SC, Ye W, et al. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst Rev. 2018 May 31;5:CD000146.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000146.pub5/full
http://www.ncbi.nlm.nih.gov/pubmed/29852054?tool=bestpractice.com
[132]Rigotti NA, Clair C, Munafò MR, et al. Interventions for smoking cessation in hospitalised patients. Cochrane Database Syst Rev. 2012 May 16;(5):CD001837.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001837.pub3/full
http://www.ncbi.nlm.nih.gov/pubmed/22592676?tool=bestpractice.com
[133]Howes S, Hartmann-Boyce J, Livingstone-Banks J, et al. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2020 Apr 22;(4):CD000031.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000031.pub5/full
http://www.ncbi.nlm.nih.gov/pubmed/32319681?tool=bestpractice.com
[ ![]() ]
What are the effects of adding bupropion or fluoxetine to other treatments compared with using other treatments alone for people trying to quit smoking?/cca.html?targetUrl=https://www.cochranelibrary.com/cca/doi/10.1002/cca.4337/fullსწორი პასუხის ჩვენება
]
What are the effects of adding bupropion or fluoxetine to other treatments compared with using other treatments alone for people trying to quit smoking?/cca.html?targetUrl=https://www.cochranelibrary.com/cca/doi/10.1002/cca.4337/fullსწორი პასუხის ჩვენება
წინასაოპერაციო ვარჯიშმა ფიზიკური დატვირთვით დააქვეითა პოსტოპერაციული კარდიალური გართულებები მცირე რანდომიზებული კონტროლირებადი კვლევების მიხედვით.პაციენტებში,რომლებმაც გადაიტანეს ღია ან ენდოვასკულარული AAA პლასტიკა, თუმცა კოხრეინის მიმოხილვამ და ოპერაციამდე პრეჰაბილიტაციის (სავარჯიშო ტრენინგის) ცალკეული სისტემატური მიმოხილვამ არ აჩვენა რაიმე შედეგის სარგებელი.[191]Barakat HM, Shahin Y, Khan JA, et al. Preoperative supervised exercise improves outcomes after elective abdominal aortic aneurysm repair: a randomized controlled trial. Ann Surg. 2016 Jul;264(1):47-53. http://www.ncbi.nlm.nih.gov/pubmed/26756766?tool=bestpractice.com [192]Fenton C, Tan AR, Abaraogu UO, et al. Prehabilitation exercise therapy before elective abdominal aortic aneurysm repair. Cochrane Database Syst Rev. 2021 Jul 8;7(7):CD013662. https://www.doi.org/10.1002/14651858.CD013662.pub2 http://www.ncbi.nlm.nih.gov/pubmed/34236703?tool=bestpractice.com [193]Bonner RJ, Wallace T, Jones AD, et al. The content of pre-habilitative interventions for patients undergoing repair of abdominal aortic aneurysms and their effect on post-operative outcomes: a systematic review. Eur J Vasc Endovasc Surg. 2021 May;61(5):756-65. https://www.doi.org/10.1016/j.ejvs.2021.01.043 http://www.ncbi.nlm.nih.gov/pubmed/33678532?tool=bestpractice.com მიუხედავად იმისა, რომ წინასაოპერაციო ვარჯიში შეიძლება სასარგებლო იყოს პაციენტებისთვის, რომლებიც გადიან AAA-ს პლასტიკას, საჭიროა შემდგომი გამოკვლევა RCT-ებით, სანამ ის უფრო ფართოდ იქნება რეკომენდებული.[194]Wee IJY, Choong AMTL. A systematic review of the impact of preoperative exercise for patients with abdominal aortic aneurysm. J Vasc Surg. 2020 Jun;71(6):2123-31.e1. https://www.doi.org/10.1016/j.jvs.2018.09.039 http://www.ncbi.nlm.nih.gov/pubmed/30606665?tool=bestpractice.com
პერიოპერაციული სტატინების გამოყენება ანელებს ანევრიზმის ზრდას, ამცირებს რღვევის რისკს და ამცირებს სიკვდილიანობას AAA-ს პლასტიკის ან გახეთქილი AAA-სგან.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com სტატინები უნდა დაინიშნოს ქირურგიულ ჩარევამდე სულ მცირე 1 თვით ადრე, რათა შემცირდეს გულსისხლძარღვთა მიზეზით სიკვდილობა. სტატინები გრძელდება განუსაზღვრელი ვადით.[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com [136]Risum Ø, Sandven I, Sundhagen JO, et al. Editor's choice - effect of statins on total mortality in abdominal aortic aneurysm repair: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2021 Jan;61(1):114-20. https://www.doi.org/10.1016/j.ejvs.2020.08.007 http://www.ncbi.nlm.nih.gov/pubmed/32928667?tool=bestpractice.com
პაციენტებს AAA-ით აქვთ მაღალი რისკი გულ-სისხლძარღვთა დაავადებების სერიოზული გართულებების მხრივ. არსებობს შეზღუდული მტკიცებულება, მაგრამ რაიმე უკუჩვენების არარსებობის შემთხვევაში, AAA-ს მქონე პაციენტებმა უნდა მიიღონ ერთჯერადი ანტითრომბოციტული თერაპია (ასპირინი ან კლოპიდოგრელი).[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [137]Aboyans V, Bauersachs R, Mazzolai L, et al. Antithrombotic therapies in aortic and peripheral arterial diseases in 2021: a consensus document from the ESC working group on aorta and peripheral vascular diseases, the ESC working group on thrombosis, and the ESC working group on cardiovascular pharmacotherapy. Eur Heart J. 2021 Oct 14;42(39):4013-24. https://www.doi.org/10.1093/eurheartj/ehab390 http://www.ncbi.nlm.nih.gov/pubmed/34279602?tool=bestpractice.com დააკვირდეთ პაციენტებს პერიოპერაციულ პერიოდში[9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
ჰიპერტენზია უნდა გაკონტროლდეს გულსისხლძარღვთა ავადობის შესამცირებლად.[4]Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482. https://www.doi.org/10.1161/CIR.0000000000001106 http://www.ncbi.nlm.nih.gov/pubmed/36322642?tool=bestpractice.com [9]Wanhainen A, Verzini F, Van Herzeele I, et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019 Jan;57(1):8-93. https://www.ejves.com/article/S1078-5884(18)30698-1/fulltext http://www.ncbi.nlm.nih.gov/pubmed/30528142?tool=bestpractice.com
პერიოპერაციული ანტიბიოტიკოთერაპია
მკურნალობა, რომელიც რეკომენდებულია <strong>ყველა</strong> პაციენტისთვის შერჩეულ ჯგუფში
ჩაუტარდა პერიოპერაციული ანტიბიოტიკოთერაპია. ფართო სპექტრის ანტიბიოტიკებით პროფილაქტიკა აუცილებელია, ადგილობრივი პროტოკოლის თანახმად.
აირჩიეთ პაციენტების ჯგუფი ჩვენი რეკომენდაციების სანახავად
მიაქციეთ ყურადღება, რომ ფორმულაცია/შეყვანის გზა და დოზირება შეიძლება განსხვავებული იყოს მედიკამენტების დასახელების და ბრენდების, წამლების ფორმულარის ან გეოგრაფიული ადგილმდებარეობის მიხედვით. მკურნალობის შესახებ რეკომენდაციები სპეციფიკურია პაციენტის ჯგუფების მიხედვით. იხილეთ გაფრთხილება
ამ მასალის გამოყენება ექვემდებარება ჩვენს განცხადებას