ანამნეზი
კლინიცისტებს შესაძლოა ქონდეთ ეჭვი PCP-ზე აივ-დადებითი მოზრდილი ან მოზარდი პაციენტების მკურნალობისას, განსაკუთრებით, თუ ვერ ემორჩილება ანტირეტროვირუსულ მკურნალობას (ART) ან PCP პროფილაქტიკას, ადრე ქონდათ PCP-ს ეპიზოდი და/ან აქვთ CD4 უჯრედების რაოდენობა <200 უჯრედი/მიკროლიტრი.[60]Katz MH, Baron RB, Grady D. Risk stratification of ambulatory patients suspected of Pneumocystis pneumonia. Arch Intern Med. 1991 Jan;151(1):105-10.
http://www.ncbi.nlm.nih.gov/pubmed/1985585?tool=bestpractice.com
აივ-დადებითი დედების აივ-განუსაზღვრელი ჩვილები, რომლებსაც რესპირატორული სიმპტომები აქვთ, უნდა შემოწმდენენ პნევმოცისტურ პნევმონიაზე.
პაციენტების სხვა ჯგუფები, რომლებშიც არსებობს ეჭვი PCP-ზე, იმუნოკომპრომისული პირები არიან, რომლებსაც ანამნეზში აქვთ:[31]Stern A, Green H, Paul M, et al. Prophylaxis for Pneumocystis pneumonia (PCP) in non-HIV immunocompromised patients. Cochrane Database Syst Rev. 2014 Oct 1;(10):CD005590.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005590.pub3/full
http://www.ncbi.nlm.nih.gov/pubmed/25269391?tool=bestpractice.com
[47]Taplitz RA, Kennedy EB, Bow EJ, et al. Antimicrobial prophylaxis for adult patients with cancer-related immunosuppression: ASCO and IDSA clinical practice guideline update. J Clin Oncol. 2018 Oct 20;36(30):3043-54.
https://ascopubs.org/doi/10.1200/JCO.18.00374?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub++0pubmed
http://www.ncbi.nlm.nih.gov/pubmed/30179565?tool=bestpractice.com
[48]Tomblyn M, Chiller T, Einsele H, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol Blood Marrow Transplant. 2009 Oct;15(10):1143-238.
https://www.bbmt.org/article/S1083-8791(09)00300-0/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/19747629?tool=bestpractice.com
[49]Fishman JA, Gans H, AST Infectious Diseases Community of Practice. Pneumocystis jiroveci in solid organ transplantation: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019 Sep;33(9):e13587.
http://www.ncbi.nlm.nih.gov/pubmed/31077616?tool=bestpractice.com
ჰემატოლოგიური ავთვისებიანი მდგომარეობა
ჰემატოპოეტური უჯრედების ტრანსპლანტაცია
სხვა ავთვისებიანი დაავადებები, რომელთა სამკურნალოდ დანიშნული ქიმიოთერაპიის რეჟიმი დაკავშირებულია პნევმოცისტური პნევმონიის >3.5%-იან რისკთან
მკვრივი ორგანოების ტრანსპლანტაცია
კორტიკოსტეროიდების ქრონიკული გამოყენება სხვა იმუნოსუპრესიულ მედიკამენტებთან და მათ გარეშეც
ზოგიერთი პირველადი იმუნოდეფიციტური დაავადება (მაგ. მძიმე კომბინირებული იმუნოდეფიციტი).
ატიპური პნევმონიის მქონე პაციენტებში აივ რისკ-ფაქტორების შეფასება და აივ ტესტის ჩატარება შესაძლოა დაგვეხმაროს PCP-ს რისკის მქონე პაციენტების აღმოჩენაში.
აივ-დადებით PCP პაციენტების გამოვლინება თანდათანობით იწყება დაღლილობით, ცხელებით, შეციებით, ოფლიანობით, არაპროდუქტიული ხველით და დისპნოეთი რამდენიმე კვირის განმავლობაში. PCP-თან დაკავშირებული სხვა ნიშნებია ანამნეზში განმეორებითი ბაქტერიული პნევმონიები, წონაში კლება და პირის ღრუს კანდიდიაზი.[43]Salzer HJF, Schäfer G, Hoenigl M, et al. Clinical, diagnostic, and treatment disparities between HIV-infected and non-HIV-infected immunocompromised patients with Pneumocystis jirovecii pneumonia. Respiration. 2018;96(1):52-65.
https://www.karger.com/Article/FullText/487713
http://www.ncbi.nlm.nih.gov/pubmed/29635251?tool=bestpractice.com
აივ-უარყოფით პაციენტებში გამოვლინება ტიპურად უფრო სწრაფად და უფრო მძიმე ფორმით ხდება.[43]Salzer HJF, Schäfer G, Hoenigl M, et al. Clinical, diagnostic, and treatment disparities between HIV-infected and non-HIV-infected immunocompromised patients with Pneumocystis jirovecii pneumonia. Respiration. 2018;96(1):52-65.
https://www.karger.com/Article/FullText/487713
http://www.ncbi.nlm.nih.gov/pubmed/29635251?tool=bestpractice.com
სიმპტომების დაწყება შესაძლოა გამოვლინდეს მაშინ, როცა იმუნოსუპრესიული მედიკამენტების ჩვეული დოზა მცირდება ან წყდება.[61]Pareja JGR, Garland R, Koziel H. Use of adjunctive corticosteroids in severe adult non-HIV Pneumocystis carinii pneumonia. Chest. 1998 May;113(5):1215-24.
http://www.ncbi.nlm.nih.gov/pubmed/9596297?tool=bestpractice.com
იშვიათად, ინფექცია იწვევს ექსტრაპულმონურ გამოვლინებებს პაციენტებში, რომლებსაც შორს წასული აივ აქვთ; თუმცა, შორს წასული შიდსის მქონე ან აივ-დადებით პაციენტებში, რომლებიც არ იღებენ პროფილაქტიკას, შესაძლოა აღინიშნებოდეს სისტემური ინფექცია მხედველობის სიმპტომებით, კოგნიტიური დარღვევებით, რაც ცენტრალურ ნერვულ სისტემას მოიცავს და კუჭ-ნაწლავის სიმპტომებით, როგორიცაა დიარეა.
კვლევები
თუ კლინიკური სურათის საფუძველზე არსებობს ეჭვი PCP-ზე და გულმკერდის რენტგენი შეესაბამება PCP-ს, დიაგნოზის დასმის დროს პირველი საფეხური უნდა იყოს ინდუცირებული ნახველის კვლევა Pneumocystis jirovecii-ის არსებობაზე.[62]Singh N, Shafer RW, Swindells S (eds). HIV clinical manual. Pittsburgh, PA: ESun Technologies; 2003. სპონტანურად ინდუცირებული ნახველის სენსიტიურობა პნევმოცისტური პნევმონიის სადიაგნოსტიკოდ დაბალია, ამიტომ ნახველი არ გამოიყენება. ინდუცირებული ნახველის ტესტირების სენსიტიურობა 50-90%-ია ნიმუშის ხარისხის, შეღებვის მეთოდის, პათოგენის რაოდენობის და დაწესებულების გამოცდილების მიხედვით.[32]Centers for Disease Control and Prevention; National Institutes of Health; HIV Medicine Association of the Infectious Diseases Society of America. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV. Pneumocystis jirovecii pneumonia. Mar 2019 [internet publication].
https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportunistic-infection/pneumocystis-pneumonia
[63]Fortun J, Navas E, Marti-Belda P, et al. Pneumocystis carinii pneumonia in HIV-infected patients: diagnostic yield of induced sputum and immunofluorescent stain with monoclonal antibodies. Eur Respir J. 1992 Jun;5(6):665-9.
http://www.ncbi.nlm.nih.gov/pubmed/1628723?tool=bestpractice.com
[64]Kovacs JA, Ng VL, Masur H, et al. Diagnosis of Pneumocystis carinii pneumonia: improved detection in sputum with use of monoclonal antibodies. N Engl J Med. 1988 Mar 10;318(10):589-93.
http://www.ncbi.nlm.nih.gov/pubmed/2449613?tool=bestpractice.com
[65]Midgley J, Parsons P, Leigh TR, et al. Increased sensitivity of immunofluorescence for detection of Pneumocystis carinii. Lancet. 1989 Dec 23-30;2(8678-8679):1523.
http://www.ncbi.nlm.nih.gov/pubmed/2574793?tool=bestpractice.com
[66]Ng VL, Virani NA, Chaisson RE, et al. Rapid detection of Pneumocystis carinii using a direct fluorescent monoclonal antibody stain. J Clin Microbiol. 1990 Oct;28(10):2228-33.
http://www.ncbi.nlm.nih.gov/pubmed/1699968?tool=bestpractice.com
თუ ნახველის ინდუქცია უარყოფითია, უნდა შესრულდეს ბრონქოსკოპიური კვლევა ბრონქოალვეოლური ლავაჟით. ბრონქოალვეოლური ლავაჟის მგრძნობელობა 90-99%-ია აივ-დადებით პაციენტებში, შესაბამისად, ის ჩვეულებრივ სრულდება ტრანსბრონქული ბიოფსიის გარეშე.[32]Centers for Disease Control and Prevention; National Institutes of Health; HIV Medicine Association of the Infectious Diseases Society of America. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV. Pneumocystis jirovecii pneumonia. Mar 2019 [internet publication].
https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportunistic-infection/pneumocystis-pneumonia
ზოგადად, თუ BAL უარყოფითია აივ-დადებით პაციენტებში, სხვა ეტიოლოგიაზე უნდა ვიფიქროთ და მკურნალობა უნდა შეწყდეს.
ტრანსბრონქული ბიოფსია შესაძლოა შესრულდეს, თუ საწყისი BAL უარყოფითია, მაგრამ კლინიკური ეჭვი PCP -ზე მაღალია ან სხვა დიაგნოზია უფრო სავარაუდო. ტრანსბრონქული ბიოფსიების სენსიტიურობა 95-100%-ია.[32]Centers for Disease Control and Prevention; National Institutes of Health; HIV Medicine Association of the Infectious Diseases Society of America. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV. Pneumocystis jirovecii pneumonia. Mar 2019 [internet publication].
https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportunistic-infection/pneumocystis-pneumonia
აივ-უარყოფით პაციენტებში ტრანსბრონქული ბიოფსია უფრო ხშირადაა აუცილებელი დიაგნოზის დასადასტურებლად, რადგანაც ლავაჟი ნაკლებად სენსიტიურია. ტრანსბრონქულ ბიოფსიას ისეთი გართულებების მაღალი რისკი აქვს, როგორიცაა სისხლდენა და პნევმოთორაქსი. პნევმოთორაქსი გამოვლინდა აივ-დადებითი პაციენტების 9%-ში, რომლებსაც ჩაუტრდა ტრანსბრონქული ბიოფსიები ერთ სერიაში, 5%-ში საჭირო გახდა პლევრული სადრენაჟო მილის ჩადგმა.[67]Harcup C, Baier HJ, Pitchenik AE. Evaluation of patients with the acquired immunodeficiency syndrome (AIDS) by fiberoptic bronchoscopy. Endoscopy. 1985 Nov;17(6):217-20.
http://www.ncbi.nlm.nih.gov/pubmed/3877629?tool=bestpractice.com
თუ კლინიკური ეჭვი პნევმოცისტურ პნევმონიაზე კვლავ მაღალია ან წინა ანალიზმა არ გამოავლინა პაციენტის დაავადების ეტიოლოგია, ფილტვის ღია ბიოფსიის ჩატარებაზე უნდა ვიფიქროთ, რათა დადასტურდეს ან გამოირიცხოს პნევმოცისტი, ასევე განისაზღვროს არის, თუ არა რაიმე სხვა პათოლოგია. ფილტვის ღია ბიოფსიის სენსიტიურობა 95-100%-ია.[32]Centers for Disease Control and Prevention; National Institutes of Health; HIV Medicine Association of the Infectious Diseases Society of America. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV. Pneumocystis jirovecii pneumonia. Mar 2019 [internet publication].
https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportunistic-infection/pneumocystis-pneumonia
შრატში მომატებულ LDH-ს (>220 საერთაშორისო ერთეული/ლ) სადიაგნოსტიკო და პროგნოზული მნიშვნელობა აქვს და LDH-ის მაღალი დონეები დაავშირებულია სიკვდილიანობის გაზრდასთან.[68]Zaman MK, White DA. Serum lactate dehydrogenase levels and Pneumocystis carinii pneumonia. Diagnostic and prognostic significance. Lancet. 1988 Nov 5;2(8619):1049-51.
http://www.ncbi.nlm.nih.gov/pubmed/3258483?tool=bestpractice.com
არტერიული სისხლის აირები იზომება სიმძიმის დასადგენად:[32]Centers for Disease Control and Prevention; National Institutes of Health; HIV Medicine Association of the Infectious Diseases Society of America. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV. Pneumocystis jirovecii pneumonia. Mar 2019 [internet publication].
https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportunistic-infection/pneumocystis-pneumonia
პნევმოცისტური პნევმონიის კლინიკური გამოვლინებების მქონე პაციენტებს, რომლებსაც გულმკერდის ნორმალური ან შეუცვლელი რენტგენი აქვთ, უნდა ჩაუტარდეთ გულმკერდის მაღალრეზოლუციური კომპიუტერული ტომოგრაფიული (HRCT) სკანირება ან ფილტვის ფუნქციური სინჯები ნახშირბადის მონოქსიდის დიფუზური ტევადობის გაზომვასთან ერთად. თუ გულმკერდის მაღალრეზოლუციურ კომპიუტერულ ტომოგრაფიაზე ვლინდება სუბპლევრული მინის ნამსხვრევისებრი დაჩრდილვები, ან მაშინ, როდესაც ნახშირბადის მონოქსიდის დიფუზური ტევადობა დაქვეითებულია, პაციენტს უნდა ჩაუტარდეს ნახველის ინდუქცია, რასაც მოსდევს ბრონქოალვეოლური ლავაჟი (თუ ნახველის ინდუქცია უარყოფითია), რადგანაც დაბურული შუშის მსგავსი გამკვრივებების და ნახშირბადის მონოქსიდის დიფუზური დაქვეითებული ტევადობა მგრძნობიარე, მაგრამ არა სპეციფიკური შედეგებია პნევმოცისტური პნევმონიის დასადგენად.[69]Gruden JF, Huang L, Turner J, et al. High-resolution CT in the evaluation of clinically suspected Pneumocystis carinii pneumonia in AIDS patients with normal, equivocal, or nonspecific radiographic findings. AJR Am J Roentgenol. 1997 Oct;169(4):967-75.
http://www.ncbi.nlm.nih.gov/pubmed/9308446?tool=bestpractice.com
[70]Huang L, Stansell J, Osmond D, et al. Performance of an algorithm to detect Pneumocystis carinii pneumonia in symptomatic HIV-infected persons. Chest. 1999 Apr;115(4):1025-32.
http://www.ncbi.nlm.nih.gov/pubmed/10208204?tool=bestpractice.com
[71]Sankary RM, Turner J, Lipavsky A, et al. Alveolar-capillary block in patients with AIDS and Pneumocystis carinii pneumonia. Am Rev Respir Dis. 1988 Feb;137(2):443-9.
http://www.ncbi.nlm.nih.gov/pubmed/3257662?tool=bestpractice.com
თუ ორივე ანალიზი უარყოფითია, უნდა ვიფიქროთ სხვა ეტიოლოგიაზე და საჭიროა ჩატარდეს შესაბამისი დიაგნოსტიკური ტესტები. თუ Pneumocystis jirovecii-ის თითოეული დიაგნოსტიკური ნიმუში უარყოფითია, პაციენტს, მაღალი ალბათობით, არ აღენიშნება პნევმოცისტური პნევმონია. შესაბამისად, საჭიროა პაციენტის მონიტორინგი და სხვა ეტიოლოგიებზე ეჭვის მიტანა. კლინიკური სიტუაციის მიხედვით, შესაძლოა საჭირო გახდეს დამატებითი ტესტირება.
PCP-ს დიაგნოზი არ გამორიცხავს მეორე, კონკურენტული პროცესის შესაძლებლობას. თუმცა PCP-ს დიაგნოზის მიკროსკოპულად დადასტურებას ენიჭება უპირატესობა, რადგანაც მრავალ მდგომარეობას შესაძლებელია მსგავსი გამოვლინებები ქონდეს, PCP-ს კლინიკური გამოვლინებების მქონე პაციენტებს შესაძლებელია ჩაუტარდეთ ემპირული მკურნალობა, განსაკუთრებით იქ, სადაც ინდუცირებული ნახველის ან BAL-ის ჩასატარებლად რესურსები შეზღუდულია.
ნახველში ან BAL სითხეში Pneumocystis jirovecii-ის აღმოჩენა ხორციელდება საღებავებით, როგორიცაა ტოლუიდინის ლურჯი, გიემზა, დიფ-ქვიქი და ვერცხლის მეთენამინი. აგრეთვე შეიძლება გამოვიყენოთ ანტიგენის იმუნოფლუორესცენტული ანალიზები (ანტიგენის პირდაპირი ფლუორესცენტული ანალიზი), რომლებიც მაღალსენსიტიურია.[72]Shelhamer JH, Gill VJ, Quinn TC, et al. The laboratory evaluation of opportunistic pulmonary infections. Ann Intern Med. 1996 Mar 15;124(6):585-99.
http://www.ncbi.nlm.nih.gov/pubmed/8597323?tool=bestpractice.com
ტრანსბრონქულმა ბიოფსიებმა BAL-თან ერთად შესაძლოა გაზარდოს დიაგნოსტიკური სარგებელი.[73]Broaddus C, Dake MD, Stulbarg MS, et al. Bronchoalveolar lavage and transbronchial biopsy for the diagnosis of pulmonary infections in the acquired immunodeficiency syndrome. Ann Intern Med. 1985 Jun;102(6):747-52.
http://www.ncbi.nlm.nih.gov/pubmed/2986505?tool=bestpractice.com
Pneumocystis jirovecii-ის თუნდაც დაბალი რაოდენობის გამოვლენა შეიძლება ისეთი ანალიზებით, როგორებიცაა პოლიმერაზას ჯაჭვური რეაქცია, რეალური დროის პოლიმერაზას ჯაჭვური რეაქცია და უკუტრანსკრიპციის პოლიმერაზას ჯაჭვური რეაქცია. ამ ანალიზების და S-ადენოზილმეთიონინის პლაზმის დონის დადგენით შესაძლოა გავზარდოთ პნევმოცისტური პნევმონიის დიაგნოსტიკური მგრძნობელობა, თუმცა ეს ტესტები, ძირითადად, არ არის ხელმისაწვდომი. პოლიმერაზას ჯაჭვური რეაქციის ტექნიკები უფრო ხშირად გვაძლევს ცრუ დადებით შედეგს, ვიდრე ჰისტოქიმიური წესით ორგანიზმის შეღებვა.[74]Fillaux J, Malvy S, Alvarez M, et al. Accuracy of a routine real-time PCR assay for the diagnosis of Pneumocystis jiroveci pneumonia. J Microbiol Methods. 2008 Oct;75(2):258-61.
http://www.ncbi.nlm.nih.gov/pubmed/18606198?tool=bestpractice.com
[75]Tuncer S, Erguven S, Kocagoz S, et al. Comparison of cytochemical staining, immunofluorescence and PCR for diagnosis of Pneumocystis carinii on sputum samples. Scand J Infect Dis. 1998;30(2):125-8.
http://www.ncbi.nlm.nih.gov/pubmed/9730296?tool=bestpractice.com
[76]Larsen HH, Masur H, Kovacs JA, et al. Development and evaluation of a quantitative, touch-down, real-time PCR assay for diagnosing Pneumocystis carinii pneumonia. J Clin Microbiol. 2002 Feb;40(2):490-4.
http://www.ncbi.nlm.nih.gov/pubmed/11825961?tool=bestpractice.com
[77]Helweg-Larsen J, Jensen JS, Lundgren B. Diagnostic use of PCR for detection of Pneumocystis carinii in oral wash samples. J Clin Microbiol. 1998 Jul;36(7):2068-72.
http://www.ncbi.nlm.nih.gov/pubmed/9650964?tool=bestpractice.com
[78]Larsen HH, Huang L, Kovacs JA, et al. A prospective, blinded study of quantitative touch-down polymerase chain reaction using oral-wash samples for diagnosis of Pneumocystis pneumonia in HIV-infected patients. J Infect Dis. 2004 May 1;189(9):1679-83.
http://www.ncbi.nlm.nih.gov/pubmed/15116305?tool=bestpractice.com
[79]Skelly MJ, Holzman RS, Merali S. S-adenosylmethionine levels in the diagnosis of Pneumocystis carinii pneumonia in patients with HIV infection. Clin Infect Dis. 2008 Feb 1;46(3):467-71.
http://cid.oxfordjournals.org/content/46/3/467.long
http://www.ncbi.nlm.nih.gov/pubmed/18177224?tool=bestpractice.com
[80]Summah H, Zhu YG, Falagas ME, et al. Use of real-time polymerase chain reaction for the diagnosis of Pneumocystis pneumonia in immunocompromised patients: a meta-analysis. Chin Med J (Engl). 2013;126(10):1965-73.
http://www.ncbi.nlm.nih.gov/pubmed/23673119?tool=bestpractice.com
PCP-ს დიაგნოსტირებისთვის, აგრეთვე, დაინტერესდნენ შრატში (1,3)-ბეტა-D-გლუკანის გაზომვით, სოკოს კედლის ელემენტი.[81]Watanabe T, Yasuoka A, Tanuma J, et al. Serum (1-->3) beta-D-glucan as a noninvasive adjunct marker for the diagnosis of Pneumocystis pneumonia in patients with AIDS. Clin Infect Dis. 2009 Oct 1;49(7):1128-31.
http://cid.oxfordjournals.org/content/49/7/1128.long
http://www.ncbi.nlm.nih.gov/pubmed/19725788?tool=bestpractice.com
[82]Shimizu Y, Sunaga N, Dobashi K, et al. Serum markers in interstitial pneumonia with and without Pneumocystis jirovecii colonization: a prospective study. BMC Infect Dis. 2009 Apr 22;9:47.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2676289/?tool=pubmed
http://www.ncbi.nlm.nih.gov/pubmed/19383170?tool=bestpractice.com
[83]Desmet S, Van Wijngaerden E, Maertens J, et al. Serum (1-3)-beta-D-glucan as a tool for diagnosis of Pneumocystis jirovecii pneumonia in patients with human immunodeficiency virus infection or hematological malignancy. J Clin Microbiol. 2009 Dec;47(12):3871-4.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2786638/?tool=pubmed
http://www.ncbi.nlm.nih.gov/pubmed/19846641?tool=bestpractice.com
[84]Del Bono V, Mularoni A, Furfaro E, et al. Clinical evaluation of a (1,3)-beta-D-glucan assay for presumptive diagnosis of Pneumocystis jiroveci pneumonia in immunocompromised patients. Clin Vaccine Immunol. 2009 Oct;16(10):1524-6.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2756857/?tool=pubmed
http://www.ncbi.nlm.nih.gov/pubmed/19692624?tool=bestpractice.com
[85]Nakamura H, Tateyama M, Tasato D, et al. Clinical utility of serum beta-D-glucan and KL-6 levels in Pneumocystis jirovecii pneumonia. Intern Med. 2009;48(4):195-202.
https://www.jstage.jst.go.jp/article/internalmedicine/48/4/48_4_195/_article
http://www.ncbi.nlm.nih.gov/pubmed/19218768?tool=bestpractice.com
ამ კვლევებმა აჩვენა, რომ (1,3)-ბეტა-D-გლუკანი მნიშვნელოვნადაა მომატებული PCP-ს მქონე პაციენტებში, თუმცა უფრო ნაკლებად, ვიდრე PCP-ს მქონე აივ-უარყოფით პაციენტებში და დონეები არ იყო დაკავშირებული სიმძიმესა და მკურნალობაზე პასუხთან.[86]Huang L. Clinical and translational research in pneumocystis and pneumocystis pneumonia. Parasite. 2011 Feb;18(1):3-11.
http://www.ncbi.nlm.nih.gov/pubmed/21395200?tool=bestpractice.com
სხვადასხვა პოპულაციაში პნევმონიის დიაგნოზის დროს (1,3)-ბეტა-D-გლუკანის კვლევის მეტაანალიზმა (აივ-ინფიცირებული და აივ-არადაინფიცირებული) აჩვენა, რომ მთლიანი სენსიტიურობა და სპეციფიკურობა იყო 96% და 84%, შესაბამისად.[87]Onishi A, Sugiyama D, Kogata Y, et al. Diagnostic accuracy of serum 1,3-β-D-glucan for pneumocystis jiroveci pneumonia, invasive candidiasis, and invasive aspergillosis: systematic review and meta-analysis. J Clin Microbiol. 2012 Jan;50(1):7-15.
http://jcm.asm.org/content/50/1/7.long
http://www.ncbi.nlm.nih.gov/pubmed/22075593?tool=bestpractice.com
2015 წლის შედარებით უფრო თანამედროვა მეტა-ანალიზმა გამოავლინა მსგავსი მგრძნობელობა (92%) და სპეციფიკურობა (78%) აივ ინფიცირებულ პაციენტებში; თუმცა, აივ უარყოფით პირებში, მგრძნობელობა (85%) და სპეციფიკურობა (73%) უფრო დაბალი იყო.[88]Li WJ, Guo YL, Liu TJ, et al. Diagnosis of pneumocystis pneumonia using serum (1-3)-β-D-Glucan: a bivariate meta-analysis and systematic review. J Thorac Dis. 2015 Dec;7(12):2214-25.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4703639
http://www.ncbi.nlm.nih.gov/pubmed/26793343?tool=bestpractice.com
ერთ-ერთი დიდი კვლევისას, რომელშიც აივ-ინფიცირებული მონაწილეების (n=282) 69%-ს PCP ქონდა, სენსიტიურობა და სპეციფიკურობა იყო 92% და 65% შესაბამისად.[89]Sax PE, Komarow L, Finkelman MA, et al. Blood (1->3)-beta-D-glucan as a diagnostic test for HIV-related Pneumocystis jirovecii pneumonia. Clin Infect Dis. 2011 Jul 15;53(2):197-202.
http://cid.oxfordjournals.org/content/53/2/197.long
http://www.ncbi.nlm.nih.gov/pubmed/21690628?tool=bestpractice.com
სულ მცირე ერთი რესპირატორული სიმპტომის მქონე, შიდსის მქონე 159 პაციენტის კვლევაში, რომელთაგან 139-ს პნევმოცისტური პნევმონია ქონდა, (1,3)-ბეტა-D-გლუკანის (≥80 ნგ/მლ) სენსიტიურობა და სპეციფიკურობა იყო 92.8% და 75.0%, შესაბამისად.[90]Wood BR, Komarow L, Zolopa AR, et al. Test performance of blood beta-glucan for Pneumocystis jirovecii pneumonia in patients with AIDS and respiratory symptoms. AIDS. 2013 Mar 27;27(6):967-72.
http://www.ncbi.nlm.nih.gov/pubmed/23698062?tool=bestpractice.com
მაშინ, როცა სენსიტიურობა შესაძლოა დაგვეხმაროს PCP-ს გამორიცხვაში, როდესაც უფრო სენსიტიური ანალიზები არაა ხელმისაწვდომი, სპეციფიკურობის დაქვეითება განპირობებულია (1,3)-ბეტა-D-გლუკანის განსაზღვრით სხვა სოკოვანი ინფექციების დროს, რადგანაც (1,3)-ბეტა-D-გლუკანი არ არის პნევმოცისტებზე სპეციფიური ცილა და შესაძლოა ნაკლებ საიმედო იყოს აივ არაინფიცირებულ ადამიანებში.[Figure caption and citation for the preceding image starts]: წინა-უკანა გულმკერდის რენტგენი აჩვენებს ფილტვის მსუბუქ, რეტიკულურ, ბილატერალურ ინტერსტიციულ ინფილტრაციასმეთიუ გინგოს კოლექციიდან, UPMC [Citation ends]. [Figure caption and citation for the preceding image starts]: წინა-უკანა გულმკერდის რენტგენი აჩვენებს ფილტვის მძიმე ფორმის, ბილატერალურ ინტერსტიციულ ინფილტრაციას პნევმატოცელეებითმეთიუ გინგოს კოლექციიდან, UPMC [Citation ends].
[Figure caption and citation for the preceding image starts]: წინა-უკანა გულმკერდის რენტგენი აჩვენებს ფილტვის მძიმე ფორმის, ბილატერალურ ინტერსტიციულ ინფილტრაციას პნევმატოცელეებითმეთიუ გინგოს კოლექციიდან, UPMC [Citation ends]. [Figure caption and citation for the preceding image starts]: გულმკერდის კომპიუტერული ტომოგრაფიით ფილტვში ვლინდება ორმხრივი ინტერსტიციული ინფილტრატები და პნემვმატოცელეები (ცისტები), რაც დამახასიათებელია პნევმოცისტური პნევმონიისათვისმეთიუ გინგოს კოლექციიდან, UPMC [Citation ends].
[Figure caption and citation for the preceding image starts]: გულმკერდის კომპიუტერული ტომოგრაფიით ფილტვში ვლინდება ორმხრივი ინტერსტიციული ინფილტრატები და პნემვმატოცელეები (ცისტები), რაც დამახასიათებელია პნევმოცისტური პნევმონიისათვისმეთიუ გინგოს კოლექციიდან, UPMC [Citation ends].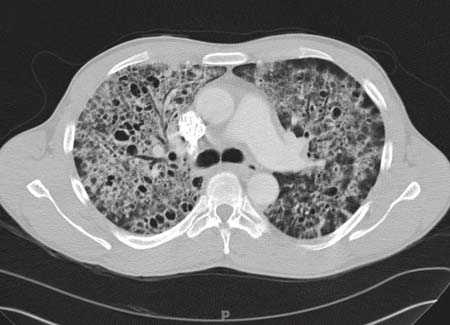 [Figure caption and citation for the preceding image starts]: ბრონქოალვეოლარული ლავაჟის (BAL) სითხის ფოტომიკროგრაფია, რომელიც გვიჩვენებს პნევმოცისტის კისტებს, გროკოტ-გომორის მეტენამინ-ვერცხლის საღებავით შავად შეღებვას (მეთილის მწვანე კონტრასტით)მეთიუ გინგოს კოლექციიდან, UPMC [Citation ends].
[Figure caption and citation for the preceding image starts]: ბრონქოალვეოლარული ლავაჟის (BAL) სითხის ფოტომიკროგრაფია, რომელიც გვიჩვენებს პნევმოცისტის კისტებს, გროკოტ-გომორის მეტენამინ-ვერცხლის საღებავით შავად შეღებვას (მეთილის მწვანე კონტრასტით)მეთიუ გინგოს კოლექციიდან, UPMC [Citation ends].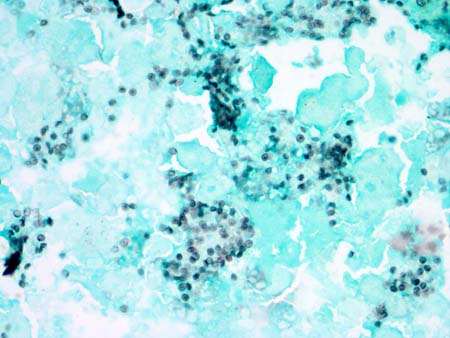
[Figure caption and citation for the preceding image starts]: პნევმოცისტური პნევმონიის დიაგნოზის ალგორითმი; ბრონქოალვეოლური ლავაჟი (BAL)მეთიუ გინგო, ადაპტირებულია სინგჰიდან, აივ-ს კლინიკური სახელმძღვანელო, 2003 [Citation ends].