A avaliação da estenose da artéria renal (EAR) inclui a consideração dos fatores na história do paciente e decisões sobre as modalidades apropriadas de estudos com imagem.
História
A idade de início da hipertensão pode ser sugestiva da etiologia subjacente da EAR:
<30 anos sugere displasia fibromuscular (DFM).[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.[16]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Apr 2;127(13):1425-43.
http://circ.ahajournals.org/content/127/13/1425.long
http://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
>55 anos sugere EAR aterosclerótica.[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.[16]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Apr 2;127(13):1425-43.
http://circ.ahajournals.org/content/127/13/1425.long
http://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
Edema pulmonar recorrente súbito ou inexplicado é sugestivo de EAR:[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.[16]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Apr 2;127(13):1425-43.
http://circ.ahajournals.org/content/127/13/1425.long
http://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
[17]Aboyans V, Ricco JB, Bartelink ME, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018 Mar 1;39(9):763-816.
https://academic.oup.com/eurheartj/article/doi/10.1093/eurheartj/ehx095/4095038/2017-ESC-Guidelines-on-the-Diagnosis-and-Treatment
http://www.ncbi.nlm.nih.gov/pubmed/28886620?tool=bestpractice.com
[18]Davenport A, Anker SD, Mebazaa A, et al.; Acute Dialysis Quality Initiative (ADQI) Consensus Group. ADQI 7: the clinical management of the Cardio-Renal syndromes: work group statements from the 7th ADQI consensus conference. Nephrol Dial Transplant. 2010 Jul;25(7):2077-89.
https://academic.oup.com/ndt/article/25/7/2077/1874047/ADQI-7-the-clinical-management-of-the-Cardio-Renal
http://www.ncbi.nlm.nih.gov/pubmed/20494894?tool=bestpractice.com
Hipertensão (acelerada, maligna ou resistente)
Pacientes com EAR aterosclerótica ou DFM podem apresentar hipertensão grave, progressiva e/ou difícil de controlar, às vezes causando danos ao órgão-alvo.[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.[16]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Apr 2;127(13):1425-43.
http://circ.ahajournals.org/content/127/13/1425.long
http://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
[19]Hicks CW, Clark TWI, Cooper CJ, et al. Atherosclerotic renovascular disease: a KDIGO (Kidney Disease: Improving Global Outcomes) controversies conference. Am J Kidney Dis. 2022 Feb;79(2):289-301.
https://www.doi.org/10.1053/j.ajkd.2021.06.025
http://www.ncbi.nlm.nih.gov/pubmed/34384806?tool=bestpractice.com
Disfunção renal ou lesão renal aguda:
A disfunção renal inexplicada pode ser resultante de estenose progressiva ou de danos aos órgãos-alvo relacionados à hipertensão.[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006 Mar 21;113(11):e463-654.
http://circ.ahajournals.org/content/113/11/e463.long
http://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.
A lesão renal aguda pode ser observada em alguns pacientes com EAR bilateral ou EAR de um único rim em funcionamento após o início de um inibidor de enzima conversora da angiotensina (ECA) ou antagonista do receptor de angiotensina II.[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006 Mar 21;113(11):e463-654.
http://circ.ahajournals.org/content/113/11/e463.long
http://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.[19]Hicks CW, Clark TWI, Cooper CJ, et al. Atherosclerotic renovascular disease: a KDIGO (Kidney Disease: Improving Global Outcomes) controversies conference. Am J Kidney Dis. 2022 Feb;79(2):289-301.
https://www.doi.org/10.1053/j.ajkd.2021.06.025
http://www.ncbi.nlm.nih.gov/pubmed/34384806?tool=bestpractice.com
Os fatores clínicos que predispõem à EAR aterosclerótica incluem:[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006 Mar 21;113(11):e463-654.
http://circ.ahajournals.org/content/113/11/e463.long
http://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
[19]Hicks CW, Clark TWI, Cooper CJ, et al. Atherosclerotic renovascular disease: a KDIGO (Kidney Disease: Improving Global Outcomes) controversies conference. Am J Kidney Dis. 2022 Feb;79(2):289-301.
https://www.doi.org/10.1053/j.ajkd.2021.06.025
http://www.ncbi.nlm.nih.gov/pubmed/34384806?tool=bestpractice.com
Doença arterial coronariana (DAC) multivasos
Outra doença vascular periférica (DVP)
Insuficiência cardíaca congestiva (ICC) inexplicada
Angina refratária
Dislipidemia
Tabagismo (relacionado à etiologia de EAR aterosclerótica e DFM)[1]Safian RD, Textor SC. Renal-artery stenosis. N Engl J Med. 2001 Feb 8;344(6):431-42.
http://www.ncbi.nlm.nih.gov/pubmed/11172181?tool=bestpractice.com
[14]Gornik HL, Persu A, Adlam D, et al. First International Consensus on the diagnosis and management of fibromuscular dysplasia. Vasc Med. 2019 Jan 16;24(2):164-89.
https://journals.sagepub.com/doi/full/10.1177/1358863X18821816
http://www.ncbi.nlm.nih.gov/pubmed/30648921?tool=bestpractice.com
Ausência de história familiar de hipertensão - pode ser sugestiva de EAR como causa da hipertensão.[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006 Mar 21;113(11):e463-654.
http://circ.ahajournals.org/content/113/11/e463.long
http://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
[13]Eisenhauer AC, White CJ. Endovascular treatment of noncoronary obstructive vascular disease. In: Libby P, Bonow RO, Mann DL, et al., eds. Braunwald's heart disease. 8th ed. Philadelphia, PA: Elsevier Saunders; 2008:1532-5.
Exame
Como o diagnóstico conclusivo de EAR só pode ser feito com imagens, os achados sugestivos no exame físico incluem:
Hipertensão na medição da pressão arterial (PA)
Sopro abdominal: o achado de um sopro abdominal deve levantar a suspeita da presença de EAR[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006 Mar 21;113(11):e463-654.
http://circ.ahajournals.org/content/113/11/e463.long
http://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.
Outros sopros: sopros em outros vasos são frequentes devido à fisiopatologia comum e à alta prevalência de DVP coexistente.[13]Eisenhauer AC, White CJ. Endovascular treatment of noncoronary obstructive vascular disease. In: Libby P, Bonow RO, Mann DL, et al., eds. Braunwald's heart disease. 8th ed. Philadelphia, PA: Elsevier Saunders; 2008:1532-5.
Investigações gerais
Creatinina sérica para estimar a taxa de filtração glomerular[1]Safian RD, Textor SC. Renal-artery stenosis. N Engl J Med. 2001 Feb 8;344(6):431-42.
http://www.ncbi.nlm.nih.gov/pubmed/11172181?tool=bestpractice.com
Potássio sérico: hipocalemia ou potássio normal-baixo pode sugerir ativação do sistema renina-angiotensina-aldosterona.[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.
Urinálise e avaliação de sedimentos (para excluir doença glomerular): na ausência de nefropatia diabética ou nefroesclerose hipertensiva coexistente, a EAR costuma ser não proteinúrica sem anormalidades no sedimento urinário.[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006 Mar;1(2):172-81.
http://cjasn.asnjournals.org/content/1/2/172.full
http://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com
[20]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002 Nov;13 Suppl 3:S184-6.
http://jasn.asnjournals.org/content/13/suppl_3/S184.full
http://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com
A avaliação das causas secundárias de hipertensão, conforme indicado, deve ser descartada e considerada no diagnóstico diferencial: por exemplo, a relação entre aldosterona e renina (uma relação <20 descarta o hiperaldosteronismo primário).[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.
Escolha de imagens
Além dos dados laboratoriais básicos, persiste a controvérsia sobre qual modalidade de imagem é a mais adequada. Enquanto a ultrassonografia oferece uma avaliação segura e não invasiva, sua sensibilidade e especificidade são mais baixas que em outras modalidades e o seu uso fornece apenas evidências indiretas da presença de estenose. Outras técnicas não invasivas (isto é, angiotomografia ou angiografia por RM) apresentam risco associado ao uso do meio de contraste (nefropatia e fibrose sistêmica nefrogênica decorrentes de radiocontraste, respectivamente). Apesar do risco do procedimento (por exemplo, ateroembolismo e sangramento) e do risco de nefropatia decorrente do radiocontraste, a angiografia convencional tem a vantagem de ser capaz de determinar a importância clínica das lesões pela medição do gradiente de pressão em uma lesão estenótica, e a possibilidade de se realizar a terapia endovascular ao mesmo tempo. Modalidades de imagem alternativas que os especialistas podem considerar em pacientes com doença renal crônica (DRC) incluem a angiografia por ressonância magnética sem contraste[21]Utsunomiya D, Miyazaki M, Nomitsu Y, et al. Clinical role of non-contrast magnetic resonance angiography for evaluation of renal artery stenosis. Circ J. 2008 Oct;72(10):1627-30.
https://www.jstage.jst.go.jp/article/circj/72/10/72_CJ-08-0005/_pdf
http://www.ncbi.nlm.nih.gov/pubmed/18728334?tool=bestpractice.com
[22]Khoo MM, Deeab D, Gedroyc WM, et al. Renal artery stenosis: comparative assessment by unenhanced renal artery MRA versus contrast-enhanced MRA. Eur Radiol. 2011 Jul;21(7):1470-6.
http://www.ncbi.nlm.nih.gov/pubmed/21337034?tool=bestpractice.com
[23]Angeretti MG, Lumia D, Canì A, et al. Non-enhanced MR angiography of renal arteries: comparison with contrast-enhanced MR angiography. Acta Radiol. 2013 Sep;54(7):749-56.
http://www.ncbi.nlm.nih.gov/pubmed/23550187?tool=bestpractice.com
e a angiografia invasiva com dióxido de carbono (CO2).[24]Caridi JG, Stavropoulos SW, Hawkins IF Jr. CO2 digital subtraction angiography for renal artery angioplasty in high-risk patients. AJR Am J Roentgenol. 1999 Dec;173(6):1551-6.
http://www.ajronline.org/doi/pdf/10.2214/ajr.173.6.10584800
http://www.ncbi.nlm.nih.gov/pubmed/10584800?tool=bestpractice.com
[25]Lorch H, Steinhoff J, Fricke L, et al. CO2 angiography of transplanted kidneys [in German]. Rontgenpraxis. 2003;55(1):26-32.
http://www.ncbi.nlm.nih.gov/pubmed/12650035?tool=bestpractice.com
[26]Liss P, Eklöf H, Hellberg O, et al. Renal effects of CO2 and iodinated contrast media in patients undergoing renovascular intervention: a prospective, randomized study. J Vasc Interv Radiol. 2005 Jan;16(1):57-65.
http://www.ncbi.nlm.nih.gov/pubmed/15640411?tool=bestpractice.com
É recomendado começar com um exame de imagem não invasivo em pacientes com alta probabilidade clínica de EAR.
O risco do paciente é determinado pelo índice de suspeita do médico, com base nos dados demográficos do paciente (início da hipertensão com <30 ou >55 anos), comorbidades clínicas (DVP, DAC, AVC) e condição clínica (hipertensão refratária a mais de três agentes anti-hipertensivos).
Se os resultados dos exames não invasivos forem inconclusivos e a suspeita clínica de EAR for alta, exames invasivos serão recomendados.[Figure caption and citation for the preceding image starts]: Angiografia por ressonância magnética (reconstrução renderizada do volume tridimensional) em um paciente com estenose da artéria renal aterosclerótica bilateral significativa. As setas indicam estenoses bilaterais proximaisCortesia de David J. Sheehan, DO; Radiology Department, University of Massachusetts Medical Center and Medical School [Citation ends].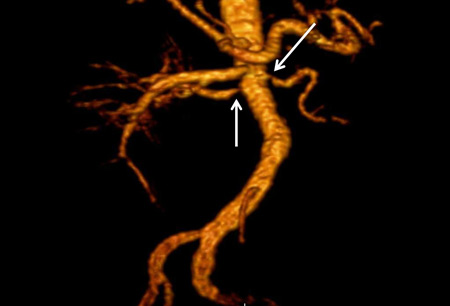 [Figure caption and citation for the preceding image starts]: Angiografia por ressonância magnética (projeção de intensidade máxima) em paciente com displasia fibromuscular das artérias renais. As setas indicam o contorno irregular característico na artéria renal direitaCortesia de Raul Galvez, MD, MPH e Hale Ersoy, MD; Department of Radiology, Brigham and Women’s Hospital, Harvard Medical School [Citation ends].
[Figure caption and citation for the preceding image starts]: Angiografia por ressonância magnética (projeção de intensidade máxima) em paciente com displasia fibromuscular das artérias renais. As setas indicam o contorno irregular característico na artéria renal direitaCortesia de Raul Galvez, MD, MPH e Hale Ersoy, MD; Department of Radiology, Brigham and Women’s Hospital, Harvard Medical School [Citation ends]. [Figure caption and citation for the preceding image starts]: Angiografia digital por subtração em paciente com estenose da artéria renal esquerda aterosclerótica significativa. Imagem A, antes da colocação do stent. Imagem B, depois da implantação bem-sucedida do stent. As setas indicam o local da estenose e da colocação do stent nas respectivas imagensCortesia de Alvaro Alonso, MD e Scott J. Gilbert, MD [Citation ends].
[Figure caption and citation for the preceding image starts]: Angiografia digital por subtração em paciente com estenose da artéria renal esquerda aterosclerótica significativa. Imagem A, antes da colocação do stent. Imagem B, depois da implantação bem-sucedida do stent. As setas indicam o local da estenose e da colocação do stent nas respectivas imagensCortesia de Alvaro Alonso, MD e Scott J. Gilbert, MD [Citation ends].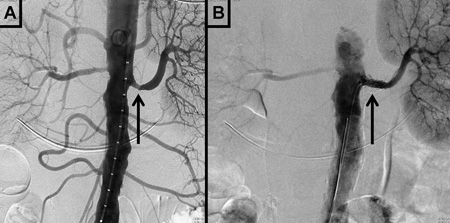
Exames de imagem não invasivos
É razoável começar com uma ultrassonografia duplex renal, seguida por angiotomografia ou angiografia por RM ou uma cintilografia renal com captopril. As sequências de angiografia por RM sem contraste podem ser consideradas em pacientes com DRC.[21]Utsunomiya D, Miyazaki M, Nomitsu Y, et al. Clinical role of non-contrast magnetic resonance angiography for evaluation of renal artery stenosis. Circ J. 2008 Oct;72(10):1627-30.
https://www.jstage.jst.go.jp/article/circj/72/10/72_CJ-08-0005/_pdf
http://www.ncbi.nlm.nih.gov/pubmed/18728334?tool=bestpractice.com
[22]Khoo MM, Deeab D, Gedroyc WM, et al. Renal artery stenosis: comparative assessment by unenhanced renal artery MRA versus contrast-enhanced MRA. Eur Radiol. 2011 Jul;21(7):1470-6.
http://www.ncbi.nlm.nih.gov/pubmed/21337034?tool=bestpractice.com
[23]Angeretti MG, Lumia D, Canì A, et al. Non-enhanced MR angiography of renal arteries: comparison with contrast-enhanced MR angiography. Acta Radiol. 2013 Sep;54(7):749-56.
http://www.ncbi.nlm.nih.gov/pubmed/23550187?tool=bestpractice.com
Ultrassonografia duplex (sensibilidade de 84% a 98%, especificidade de 62% a 99%). Pode identificar discrepância no tamanho do rim e na velocidade do fluxo sanguíneo renal.[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006 Mar;1(2):172-81.
http://cjasn.asnjournals.org/content/1/2/172.full
http://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com
[16]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Apr 2;127(13):1425-43.
http://circ.ahajournals.org/content/127/13/1425.long
http://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
[20]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002 Nov;13 Suppl 3:S184-6.
http://jasn.asnjournals.org/content/13/suppl_3/S184.full
http://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com
Os critérios de diagnóstico por ultrassonografia para estenose da artéria renal significativa são:[27]Gerhard-Herman M, Gardin JM, Jaff M, et al. Guidelines for noninvasive vascular laboratory testing: a report from the American Society of Echocardiography and the Society for Vascular Medicine and Biology. Vasc Med. 2006 Nov;11(3):183-200.
http://vmj.sagepub.com/content/11/3/183.long
http://www.ncbi.nlm.nih.gov/pubmed/17288127?tool=bestpractice.com
O índice de resistência renal >0.8 foi usado como um critério historicamente, mas como hoje se sabe que o índice de resistência é influenciado por fatores extrarrenais, como a hemodinâmica sistêmica, ele não é mais usado rotineiramente no diagnóstico de EAR.[28]Hashimoto J, Ito S. Central pulse pressure and aortic stiffness determine renal hemodynamics: pathophysiological implication for microalbuminuria in hypertension. Hypertension. 2011 Nov;58(5):839-46.
https://www.doi.org/10.1161/HYPERTENSIONAHA.111.177469
http://www.ncbi.nlm.nih.gov/pubmed/21968753?tool=bestpractice.com
[29]O'Neill WC. Renal resistive index: a case of mistaken identity. Hypertension. 2014 Nov;64(5):915-7.
https://www.doi.org/10.1161/HYPERTENSIONAHA.114.04183
http://www.ncbi.nlm.nih.gov/pubmed/25156171?tool=bestpractice.com
Angiografia por ressonância magnética contrastada com gadolínio (sensibilidade de 90% a 100%, especificidade de 76% a 94%).[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006 Mar 21;113(11):e463-654.
http://circ.ahajournals.org/content/113/11/e463.long
http://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006 Mar;1(2):172-81.
http://cjasn.asnjournals.org/content/1/2/172.full
http://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com
[16]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Apr 2;127(13):1425-43.
http://circ.ahajournals.org/content/127/13/1425.long
http://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
[20]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002 Nov;13 Suppl 3:S184-6.
http://jasn.asnjournals.org/content/13/suppl_3/S184.full
http://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com
As sequências de angiografia por RM sem contraste podem ser consideradas em pacientes com DRC.[21]Utsunomiya D, Miyazaki M, Nomitsu Y, et al. Clinical role of non-contrast magnetic resonance angiography for evaluation of renal artery stenosis. Circ J. 2008 Oct;72(10):1627-30.
https://www.jstage.jst.go.jp/article/circj/72/10/72_CJ-08-0005/_pdf
http://www.ncbi.nlm.nih.gov/pubmed/18728334?tool=bestpractice.com
[22]Khoo MM, Deeab D, Gedroyc WM, et al. Renal artery stenosis: comparative assessment by unenhanced renal artery MRA versus contrast-enhanced MRA. Eur Radiol. 2011 Jul;21(7):1470-6.
http://www.ncbi.nlm.nih.gov/pubmed/21337034?tool=bestpractice.com
[23]Angeretti MG, Lumia D, Canì A, et al. Non-enhanced MR angiography of renal arteries: comparison with contrast-enhanced MR angiography. Acta Radiol. 2013 Sep;54(7):749-56.
http://www.ncbi.nlm.nih.gov/pubmed/23550187?tool=bestpractice.com
Angiotomografia (sensibilidade de 59% a 96%, especificidade de 82% a 99%).[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006 Mar 21;113(11):e463-654.
http://circ.ahajournals.org/content/113/11/e463.long
http://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006 Mar;1(2):172-81.
http://cjasn.asnjournals.org/content/1/2/172.full
http://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com
[20]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002 Nov;13 Suppl 3:S184-6.
http://jasn.asnjournals.org/content/13/suppl_3/S184.full
http://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com
[30]Olbricht CJ, Paul K, Prokop M, et al. Minimally invasive diagnosis of renal artery stenosis by spiral computed tomography angiography. Kidney Int. 1995 Oct;48(4):1332-7.
http://www.ncbi.nlm.nih.gov/pubmed/8569096?tool=bestpractice.com
A cintilografia renal com captopril (sensibilidade de 45% a 94%, especificidade de 81% a 100%) tem um papel contemporâneo menos relevante por causa de sua complexidade, da baixa sensibilidade e da disponibilidade de exames mais fáceis e mais precisos.[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006 Mar 21;113(11):e463-654.
http://circ.ahajournals.org/content/113/11/e463.long
http://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006 Mar;1(2):172-81.
http://cjasn.asnjournals.org/content/1/2/172.full
http://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com
[20]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002 Nov;13 Suppl 3:S184-6.
http://jasn.asnjournals.org/content/13/suppl_3/S184.full
http://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com
O American College of Cardiology Foundation/American Heart Association e a European Society of Cardiology/European Stroke Association/European Society of Vascular Surgery não recomendam a cintilografia renal com captopril para diagnóstico de EAR.[16]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Apr 2;127(13):1425-43.
http://circ.ahajournals.org/content/127/13/1425.long
http://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
[17]Aboyans V, Ricco JB, Bartelink ME, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018 Mar 1;39(9):763-816.
https://academic.oup.com/eurheartj/article/doi/10.1093/eurheartj/ehx095/4095038/2017-ESC-Guidelines-on-the-Diagnosis-and-Treatment
http://www.ncbi.nlm.nih.gov/pubmed/28886620?tool=bestpractice.com
Exames invasivos
Angiografia convencional:[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006 Mar 21;113(11):e463-654.
http://circ.ahajournals.org/content/113/11/e463.long
http://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006 Mar;1(2):172-81.
http://cjasn.asnjournals.org/content/1/2/172.full
http://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com
[20]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002 Nov;13 Suppl 3:S184-6.
http://jasn.asnjournals.org/content/13/suppl_3/S184.full
http://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com
É o exame mais sensível e específico para avaliar o estreitamento anatômico da artéria renal.
Também permite a intervenção terapêutica ao mesmo tempo.
Requer cateterismo arterial e utilização de contraste.
Outras modalidades de diagnósticos podem ser utilizadas durante a angiografia invasiva (tais como a avaliação dos gradientes de pressão, o uso de fios de pressão para avaliar a fisiologia da lesão, ou a ultrassonografia intravascular). Do mesmo modo, a angiografia de dióxido de carbono pode ser realizada nos centros especializados em pacientes com DRC.[24]Caridi JG, Stavropoulos SW, Hawkins IF Jr. CO2 digital subtraction angiography for renal artery angioplasty in high-risk patients. AJR Am J Roentgenol. 1999 Dec;173(6):1551-6.
http://www.ajronline.org/doi/pdf/10.2214/ajr.173.6.10584800
http://www.ncbi.nlm.nih.gov/pubmed/10584800?tool=bestpractice.com
[25]Lorch H, Steinhoff J, Fricke L, et al. CO2 angiography of transplanted kidneys [in German]. Rontgenpraxis. 2003;55(1):26-32.
http://www.ncbi.nlm.nih.gov/pubmed/12650035?tool=bestpractice.com
[26]Liss P, Eklöf H, Hellberg O, et al. Renal effects of CO2 and iodinated contrast media in patients undergoing renovascular intervention: a prospective, randomized study. J Vasc Interv Radiol. 2005 Jan;16(1):57-65.
http://www.ncbi.nlm.nih.gov/pubmed/15640411?tool=bestpractice.com