Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
sodium restriction and diuretic therapy for ascites
Additional treatment recommended for SOME patients in selected patient group
Ascites is the most common complication of cirrhosis.
Every patient with new-onset ascites should undergo a diagnostic paracentesis: cell count with differential, albumin, and total protein should be measured in the ascitic fluid. Ascitic fluid should also be sent for culture and cytology.
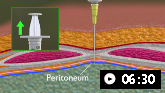
Demonstrates how to perform diagnostic and therapeutic abdominal paracentesis.
The serum-ascites albumin gradient (SAAG) should be calculated: a SAAG of ≥11 g/L with low ascitic fluid total protein is consistent with portal hypertension secondary to cirrhosis.
Treatment involves a no-added-salt diet (daily intake of not more than 5 to 6.5 g) and the use of diuretics.[101] First-line diuretic should be spironolactone due to its effects on aldosterone and maintaining normal serum potassium. Furosemide may be added to patients who do not respond to spironolactone.[101] Once-daily dosing is typically preferred. The doses of both oral diuretics can be increased simultaneously every 3-5 days (maintaining the 100 mg to 40 mg ratio) if weight loss and natriuresis are inadequate.[176] Serum sodium, potassium, and creatinine should be monitored.
Non-steroidal anti-inflammatory drugs (NSAIDs), ACE inhibitors, and other nephrotoxins should be avoided in patients with ascites.[90]
Primary options
spironolactone: 100 mg orally once daily initially, titrate as needed every 3-5 days, maximum 400 mg/day
OR
spironolactone: 100 mg orally once daily initially, titrate as needed every 3-5 days, maximum 400 mg/day
and
furosemide: 40 mg orally once daily initially, titrate as needed every 3-5 days, maximum 160 mg/day
transjugular intrahepatic portosystemic shunt (TIPS)
Patients not suitable for liver transplantation should be considered for TIPS placement.[103]
Meta-analyses indicate that TIPS is more effective than paracentesis for control of refractory ascites, but is associated with a higher incidence of hepatic encephalopathy.[103][104][105][106][107][108][109] Overall mortality does not appear to differ between the two interventions, but TIPS may confer a modest benefit with respect to transplant-free survival.[103][104][105][106][107][108][109] One Cochrane systematic review and network meta-analysis reported that the overall certainty (quality) of evidence was very low, primarily because of unclear or high risk of bias in trials assessing interventions for the treatment of refractory ascites in patients with cirrhosis.[103]
[ ![]() ]
]
Disease severity at the time of TIPS placement is an important predictive factor for outcomes.[112]
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer