Epidemiology
The epidemiology of AV block is not well characterized.[2] One study comparing the prevalence of first-degree AV block in African-American and white patients found that first-degree AV block was more prevalent in African-American patients in almost all decades of life (third through 10th).[3] In both groups, first-degree AV block became more common at age 50 years and increased with advancing age, peaking in the 10th decade for African-American patients and in the ninth decade for white patients. Another study examined 24-hour Holter monitors in 625 asymptomatic, heart-disease-free people, ages 15 to 83 years.[4] Transient type I second-degree AV block was seen in 14 (2.2%) patients, and was seen more frequently in patients with resting heart rates of <60 bpm. In a large cross-sectional study involving 10,926 Chinese participants ages ≥40 years, prevalence of first-degree AV block was found to be 3.4%.[5] In another large population based cohort study of 6146 participants from the MiniFinland Health Survey, 0.9% developed AV block in the course of 20 years.[6] First-degree AV block has been associated with about a 2-fold increase in the probability of atrial fibrillation, a 3-fold increase in the probability of pacemaker implantation, and an increase in all-cause mortality.[2][7]
Advanced AV block (usually type II second-degree and third-degree) is usually anatomically infranodal and is seen in advanced His-Purkinje disease. One study examined the prevalence of His-Purkinje disease in the Framingham population.[8] Here, QRS intervals of >0.12 seconds were significantly associated with coronary heart disease, congestive heart failure, AV block, hypertension, left ventricular hypertrophy, and ventricular extrasystoles. QRS intervals >0.12 seconds were rare before 50 to 60 years of age and were found in 11% of older men and 5% of older women. While intraventricular block does not inevitably lead to AV block, it frequently precedes the development of advanced AV block. Thus, this characterization of a wide-QRS interval population is likely similar to that of the advanced AV block population.[Figure caption and citation for the preceding image starts]: Third-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Third-degree heart block: right bundle-branch block escapeCourtesy of Dr Sanjiv Petkar; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Third-degree heart block: right bundle-branch block escapeCourtesy of Dr Sanjiv Petkar; used with permission [Citation ends].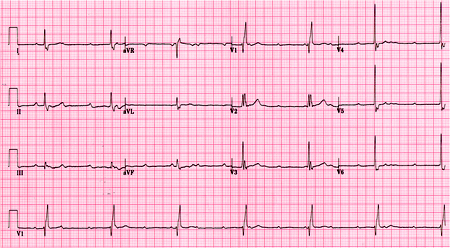 [Figure caption and citation for the preceding image starts]: Baseline ECG for a patient with third-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Baseline ECG for a patient with third-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends].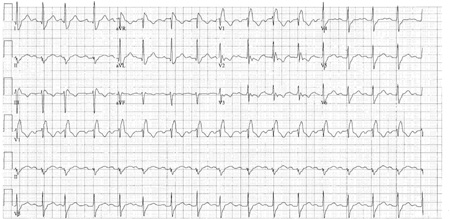
Use of this content is subject to our disclaimer