Criteria
Degrees of block[1]
First-degree AV block [Figure caption and citation for the preceding image starts]: First-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends].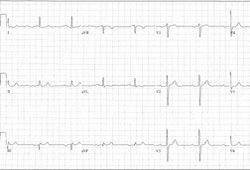
Fixed prolongation of the PR interval >0.2 seconds (or >200 milliseconds). [Figure caption and citation for the preceding image starts]: First-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends].
Severity based on the presence or absence of symptoms.
Patients with PR interval >0.30 seconds (or >300 milliseconds) may show dyspnea.
Prolonged AV delay, with an increased pulmonary capillary wedge pressure, and decreased ventricular filling leading to decreased stroke volume and cardiac output may occur.
Signs and symptoms are similar to the pacemaker syndrome experienced by some pacemaker patients.
A select number of these patients may benefit from pacemaker placement and shortening of the PR interval.
Second-degree AV block, type I [Figure caption and citation for the preceding image starts]: Type I second-degree AV block. This figure demonstrates typical features of the AV Wenckebach, including progressively shortening R-R intervals as the P-R intervals lengthen; the figure also shows grouped beating, which is also typical for AV WenckebachCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends].
Progressive prolongation of the PR interval with eventual loss of AV conduction for 1 beat.
Then, resumption of AV conduction with a PR interval that, again, progressively prolongs with eventual loss of AV conduction for 1 beat. The first sinus beat following resumption of AV conduction is conducted with a normal PR interval.
The pattern repeats.
The severity of this condition is based on the presence or absence of symptoms.
In the absence of symptoms, the prognosis is generally benign. Asymptomatic patients can be followed clinically.
Symptoms can range from those for first-degree AV block to more generalized symptoms of fatigue, presyncope, or even syncope.
In patients for whom symptoms can be attributed to the heart block and in the absence of a reversible cause, a permanent pacemaker is indicated.
Second-degree AV block, type II [Figure caption and citation for the preceding image starts]: Type II second-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends].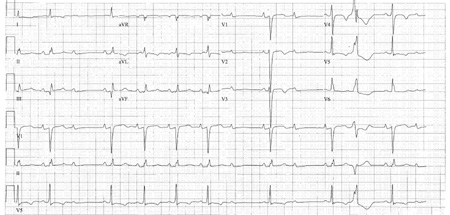
Occasional loss of AV conduction for 1 beat (during sinus rhythm, excluding premature atrial beats) preceded and followed by fixed, unchanging PR intervals.
A severe condition, and these patients are at high risk for progression to third-degree AV block.
In the absence of a reversible cause, these patients should undergo permanent pacemaker implantation.
Third-degree AV block [Figure caption and citation for the preceding image starts]: Third-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Third-degree heart block: right bundle-branch block escapeCourtesy of Dr Sanjiv Petkar; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Third-degree heart block: right bundle-branch block escapeCourtesy of Dr Sanjiv Petkar; used with permission [Citation ends].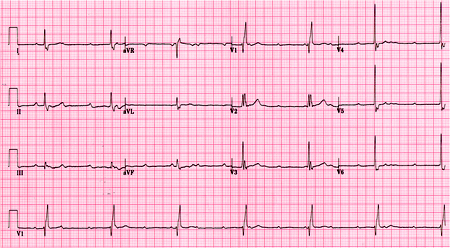
Complete, persistent loss of conduction from the atria to the ventricles.
Considered a severe condition.
In the absence of a reversible cause, these patients should undergo permanent pacemaker implantation.
High-grade AV block
The term high-grade AV block is applied to a pattern where ≥2 sinus P waves block consecutively in the context of periodic AV conduction.
Use of this content is subject to our disclaimer