Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
adenosine
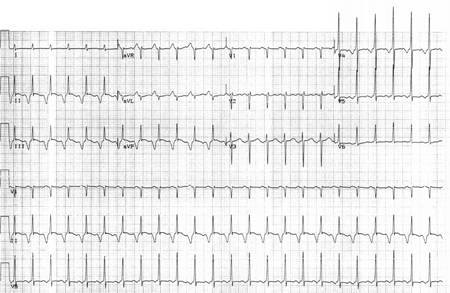
Causes AV node blockade with slowing of the ventricular response rate or cessation of the atrial tachycardia.[13] Effects are transient, and can be misleading when trying to differentiate from other forms of supraventricular tachycardia, if the focal AT terminates with adenosine.[Figure caption and citation for the preceding image starts]: Response to adenosine 6 mg intravenouslyFrom the collection of Sarah Stahmer, MD [Citation ends].
Transient slowing of the ventricular response rate with sustained atrial activity indicates flutter or focal AT. Flutter will have the characteristic saw-tooth pattern of an atrial macro-re-entrant circuit. Focal AT will show discrete P waves with an isoelectric baseline.
Lack of response to adenosine suggests either sinus tachycardia or focal AT, and strongly suggests that the rhythm is not re-entrant supraventricular tachycardia or atrial flutter.
Some forms of atrial tachycardia will break in response to adenosine.[17]
Primary options
adenosine: adults: 6 mg/dose intravenously initially, followed by 12 mg/dose in 1-2 minutes if no effect, may repeat 12 mg/dose once more in 1-2 minutes if no effect, maximum 30 mg/total dose
supportive care
Digoxin toxicity should be suspected if there is a history of congestive heart failure, the patient is taking digoxin, and the rhythm is atrial tachycardia with evidence of atrio-ventricular blockade.
When atrial tachycardia is a manifestation of digoxin toxicity, treatment is aimed at supportive care, withholding digoxin, optimising volume status, and replacing potassium if there is a deficit.[Figure caption and citation for the preceding image starts]: Focal atrial tachycardia in an 88-year-old woman with 2:1 AV nodal block in the setting of digoxin therapy and potassium 2.8 mmol/L (2.8 mEq/L)From the collection of Sarah Stahmer, MD [Citation ends].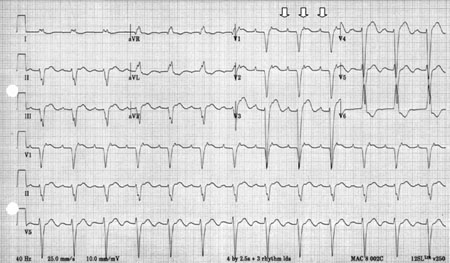
This approach is usually sufficient for restoring sinus rhythm.
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer