Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
anterior nasal packing
If you cannot identify the exact site of the bleeding, treat active bleeding that is not controlled by nasal pressure with nasal packing.[8][23] With adequate resources, you can perform anterior nasal packing in outpatient offices or emergency departments.[8]
In most cases, use nonresorbable packing. There are 2 types of packing method, traditional packing and a variety of gauze dressings, polymers, and inflatable balloons available in different sizes.[8]
Traditional packing involves horizontal layering of 12-mm (half-inch) cotton gauze saturated with petroleum jelly or antibiotic ointment.[8] The newer options are more convenient and easier to position than traditional packing, particularly for physicians who infrequently place nasal packing. Because of concerns that packing material may become displaced, some patients are managed in the hospital, but uncomplicated patients with nosebleeds controlled with nonresorbable anterior packing can usually be managed as outpatients, depending on local protocols.[8][30] Remove all types of nonresorbable packings at some point after achieving sustained control of nasal hemorrhage.[8] The pack is usually removed at 48-72 hours.[8] This allows: 1) healing of the original bleeding site; 2) remucosalization of any secondary sites from pack insertion trauma; 3) regeneration of functional platelets or clotting factors in patients on medications that impair coagulation.
As epistaxis generally originates on one side, packing is unilateral. Bilateral packing is only indicated in the unusual situation of true hemorrhage from both sides, or when the history and examination fail to identify whether the bleeding is from the right or the left. In practice, nonspecialists often resort to bilateral packing as it is difficult to determine accurately the true site of the bleed.

Demonstrates insertion of an inflatable anterior nasal pack and a nasal tampon.
Use resorbable packing (that does not need to be removed) for a patient with a suspected bleeding disorder, on antiplatelet or anticoagulant medication; vascular abnormalities such as hereditary hemorrhagic telangiectasia; or for a young child.[8]
A variety of resorbable materials is available, including oxidized regenerated cellulose, synthetic polyurethane sponge, chitosan-based materials, purified porcine skin and gelatin granules and hemostatic gelatin thrombin matrices, carboxymethylcellulose gel, hyaluronic acid, and carboxymethylcellulose.[8]
Choose the specific packing based on local availability and experience; there is limited comparative evidence to support the use of one material over any other.[8]
clear nose ± vasoconstrictor/anesthetic ± cautery
Remove any blood clot (if present) because blood clot may promote fibrinolysis.[8] Perform anterior rhinoscopy with a nasal speculum (or otoscope, particularly in children) to identify any bleeding source on the anterior nasal septum, inferior and middle turbinates, floor of the nose, and anterior nasal mucosa.[8]
Consider applying a combination of topical anesthetic (e.g., lidocaine) and vasoconstrictor (decongestant) at this stage.[8] Topical anesthetic makes the procedure more comfortable for the patient and less stressful for the physician. Some physicians prepare a mixture of anesthetic and decongestant in the office or emergency department. For the decongestant, use oxymetazoline rather than phenylephrine as the latter seems more likely to cause hypertension or possibly angina in susceptible patients. Some physicians simply remove the top from a spray bottle of oxymetazoline, add an equal volume of the lidocaine, and replace the top; however, seek specialist advice.
Active bleeding may necessitate rapid alternation between clearing of blood and liberal application of the topical vasoconstrictor and anesthetic.
Next, place small neurosurgical pledgets or strips of cotton well saturated with the mixture horizontally in the nose with bayonet forceps, and leave for 10 to 15 minutes. Ask the patient to compress their nose if necessary. [Figure caption and citation for the preceding image starts]: Nasal pledgets for application of decongestant and local anestheticFrom the collection of David A. Randall, Springfield Ear Nose Throat and Facial Plastic Surgery, MO [Citation ends].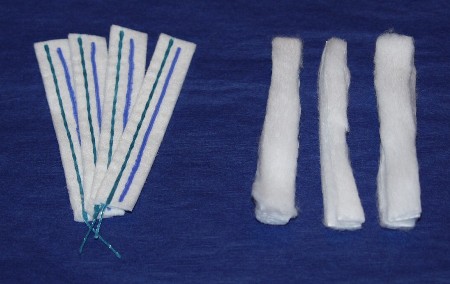
Treat patients with an identified bleeding site with one or more of the following options, as appropriate: topical vasoconstrictors (including oxymetazoline, phenylephrine, epinephrine, or cocaine), nasal cautery, and moisturizing or lubricating agents.[8] Moisturizing and lubricating agents would not usually be used for an active bleed, but would most commonly be applied after cessation of bleeding following cautery and/or vasoconstrictors.[8]
Combinations of several methods are often used; with little evidence comparing options, the American Academy of Otolaryngology guideline refrains from recommending a specific order for these interventions.[8]
The American Academy of Otolaryngology guideline recognizes that the British Rhinological Society recommends that vasoconstrictors should be used prior to cautery, and that cautery of an identified bleeding site should be first-line treatment; however, the US guideline notes that these recommendations were based on limited evidence.[28] Give oxymetazoline or phenylephrine as an intranasal spray or on a cotton pledget, but be cautious in patients with hypertension, cardiac disease, or cerebrovascular conditions, as vasoconstrictors may be associated with cardiac and other complications.
The American Academy of Otolaryngology guideline does not specify a preference for either the chemical or electrical method of cautery.[8] Silver nitrate, chromic acid, or trichloroacetic acid can be used for chemical cautery.[8] However, electrocautery is suggested to be more effective than chemical cautery if the relevant resources and expertise are available.[28]
Perform electrocautery for brisker bleeding that is resistant to silver nitrate treatment. This procedure is usually reserved for the ear, nose, and throat (ENT) specialist. It requires injection of local anesthetic plus vasoconstrictor (e.g., lidocaine with epinephrine), in addition to topical anesthetic. Monopolar and bipolar cautery are both effective. Suction monopolar cautery (if available) evacuates blood and enhances effect, as cautery is ineffective in a wet, blood-filled field. Provide routine post-treatment instructions.
Although most frequently used for office treatment of recurrent epistaxis when bleeding is quiescent, use silver nitrate cautery to treat minor anterior active epistaxis if you have identified a specific site.[8]
Silver nitrate is applied via commercially manufactured sticks or applicators. This compound degrades over time and must be kept in an airtight, lightproof container. Lack of evident activity may indicate the need to use fresher silver nitrate.
The technique for anterior nasal cautery is suggested as follows:
1) Anesthetize the bleeding site adequately; recommendations do not specify a preference for topical or injected anesthetic agents.[8] Lidocaine or tetracaine are common options.[8] Lidocaine can be injected into the nasal septum or administered topically via spray or on pledgets.[8]
2) Apply the cauterizing agent to specific vessels or hemorrhagic areas of concern, and remove excess with a cotton tip applicator.
3) The patient may find treatment uncomfortable even with adequate application of topical vasoconstrictor and anesthetic.
4) Apply petroleum jelly afterward for moisturization.
5) Avoid cautery at the same location on both sides of the septum. This deprives the septal cartilage of its blood supply (from the mucosal covering) and may result in septal perforation if done bilaterally.
unilateral or bilateral anterior packing
Use anterior nasal packing for active bleeding when cautery has been ineffective. There are 2 types of packing method, traditional packing and a variety of gauze dressings, polymers, and inflatable balloons available in different sizes.[8]
Traditional packing involves horizontal layering of 12-mm (half-inch) cotton gauze saturated with petroleum jelly or antibiotic ointment.[8] The newer options are more convenient and easier to position than traditional packing, particularly for physicians who infrequently place nasal packing. Because of concerns that packing material may become displaced, some patients are managed in the hospital, but uncomplicated patients with nosebleeds controlled with nonresorbable anterior packing can usually be managed as outpatients, depending on local protocols.[8][30] Remove all types of nonresorbable packings at some point after achieving sustained control of nasal hemorrhage.[8] The pack is usually removed at 48-72 hours.[8] This allows: 1) healing of the original bleeding site; 2) remucosalization of any secondary sites from pack insertion trauma; 3) regeneration of functional platelets or clotting factors in patients on medications that impair coagulation.
As epistaxis generally originates on one side, packing is unilateral. Bilateral packing is only indicated in the unusual situation of true hemorrhage from both sides, or when the history and examination fail to identify whether the bleeding is from the right or the left. In practice, nonspecialists often resort to bilateral packing as it is difficult to determine accurately the true site of the bleed.
Demonstrates insertion of an inflatable anterior nasal pack and a nasal tampon.
posterior packing
Perform posterior packing in an emergency department or hospital setting. Care of patients requiring this level of packing should involve an otolaryngology attending.[8]
Anterior-posterior nasal packing is indicated: 1) for known posterior bleeding; 2) in case of failure of a properly placed anterior pack to control hemorrhage.
Use anterior packing to reinforce posterior packing; the pressure at the posterior choanal area prevents anterior blood flow.
A variety of posterior pack options exist, although the methods described below provide both effectiveness and ease of placement. These are: 1) the double-balloon epistaxis device; 2) the traditional gauze anterior pack with the Foley urinary catheter placed posteriorly.
See the Management Approach section of this topic for details of how to place these packs.
[Figure caption and citation for the preceding image starts]: Anterior-posterior traditional Foley catheter-gauze packFrom the collection of David A. Randall, Springfield Ear Nose Throat and Facial Plastic Surgery, MO [Citation ends].
There has been concern about posterior packs causing hypoxia, and the need for intensive cardiorespiratory monitoring while the packs remain in place.[8] Some authors recommend observation of patients in the intensive care unit while posterior packing is in place, while others feel that this is appropriate specifically for older people and patients with comorbidities.
Remove packing after 2 to 3 days to allow healing of the original and possibly secondary (from excoriation of packing placement) bleeding sites.[8]
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer