Tests
1st tests to order
serum bilirubin
Test
Levels usually range from 2 to 5 mg/dL, but levels as high as 25 mg/dL have been reported.[32] The serum bilirubin concentration often fluctuates and occasionally bilirubin can be within normal limits.
Result
elevated, with increased plasma conjugated bilirubin
serum alkaline phosphatase
Test
Helps to differentiate from other causes of jaundice.[29]
Result
normal
serum liver aminotransferases (aspartate aminotransferase and alanine aminotransferase)
Test
Helps to differentiate from other causes of jaundice.[31]
Result
normal; occasionally there may be mild elevation of alanine aminotransferase(<2 times the upper limit of normal)
serum albumin
Test
Helps to differentiate from other causes of jaundice.
Result
normal
serum gamma-glutamyl transferase
Test
Helps to differentiate from other causes of jaundice.[29]
Result
normal
serum bile acids
Test
Fasting and postprandial levels of common bile acids are normal. Mild elevations have been described in occasional patients.
Result
normal
clotting profile
Test
Deranged clotting is not a feature of DJS, but clotting should be checked in any patient with jaundice to help differentiate from other causes.
Result
normal
Tests to consider
urinary coproporphyrin I to III ratio
Test
Total coproporphyrin levels are increased in several conditions but the proportion of isomer I in urine is almost always less than 65%. In DJS, more than 80% is excreted as coproporphyrin I, which is virtually diagnostic of DJS.[33]
Healthy neonates have been shown to have impressive elevations of urinary coproporphyrin levels, with more than 80% as isomer I during the first 2 days of life; but by day 10, the levels decrease to overlap normal adult values.[33][35]
Result
increased, total urinary coproporphyrin excretion is normal or moderately increased
99mTc hepatobiliary imino-diacetic acid (HIDA) scan (cholescintigraphy)
Test
In a healthy person, images of the biliary ducts and gallbladder are obtained within 30 minutes after injection with 99mTc HIDA; good excretion into the intestinal tract is seen in less than 60 minutes. In DJS, the uptake of the radionuclide by the liver is excellent, but the excretion into the biliary tract is impaired. Thus, a unique cholescintigram is obtained, which is a combination of intense and prolonged visualization of the liver with delayed visualization of the gallbladder and common bile duct. Sometimes the gallbladder and the biliary tract are not visualized at all.[30]
This scan can be useful if the diagnosis is unclear or if other conditions are suspected.[30]
Result
intense and prolonged visualization of the liver with delayed visualization of the gallbladder and common bile duct
liver biopsy
Test
A striking characteristic of DJS is the brown to black discoloration of the liver. These pigments may accumulate in the liver because of impaired secretion of various metabolites from the hepatocyte into the bile. This pigment disappears from the liver during acute viral hepatitis, with subsequent reappearance.[5][24][25][26][27]
A percutaneous liver biopsy is recommended in some patients to confirm the diagnosis of DJS and exclude any concomitant liver pathology.
Urinary coproporphyrin is a surrogate marker rather than a definitive test. DJS is an extremely rare condition; hence, a definitive investigation that will confirm the diagnosis and exclude other conditions will be helpful to reassure the patients as to the benign nature of this illness.[Figure caption and citation for the preceding image starts]: Masson-Fontana stain showing the pigment in a patient with DJSPersonal collection of Professor Bernard Portmann, King's College Hospital, London, with permission [Citation ends].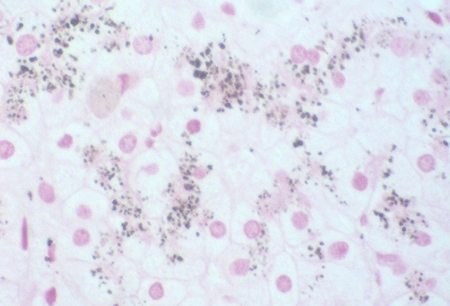 [Figure caption and citation for the preceding image starts]: Immunohistochemistry for canalicular multispecific organic anion transporter in patient showing the pigment, but no canalicular structuresPersonal collection of Professor Bernard Portmann, King's College Hospital, London, with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Immunohistochemistry for canalicular multispecific organic anion transporter in patient showing the pigment, but no canalicular structuresPersonal collection of Professor Bernard Portmann, King's College Hospital, London, with permission [Citation ends].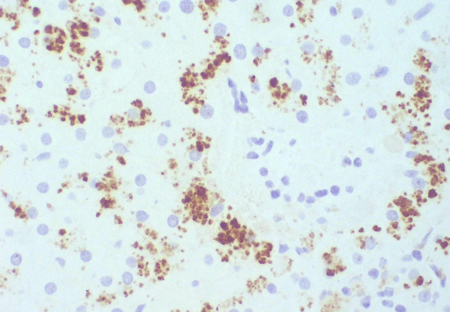 [Figure caption and citation for the preceding image starts]: Immunohistochemistry for canalicular multispecific organic anion transporter in a control, showing no pigment, but irregularly branching canalicular structures can be seenPersonal collection of Professor Bernard Portmann, King's College Hospital, London, with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Immunohistochemistry for canalicular multispecific organic anion transporter in a control, showing no pigment, but irregularly branching canalicular structures can be seenPersonal collection of Professor Bernard Portmann, King's College Hospital, London, with permission [Citation ends].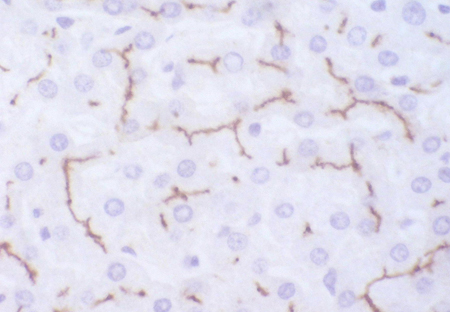
Result
coarsely granulated pigment in the hepatocyte lysosomes with normal liver histology
mutational analysis of the ABCC2 gene
Test
Mutational analysis of the ABCC2 gene (encoding multi-drug resistance-associated protein 2 [MRP2]), using next-generation sequencing and Sanger sequencing, has been reported as a potential diagnostic tool in the work-up of patients with suspected DJS.[31][36][37]
If there are existing genetic test results, do not perform repeat testing unless there is uncertainty about the existing result, e.g., the result is inconsistent with the patient’s clinical presentation or the test methodology has changed.[38]
Result
presence of a mutation in the ABCC2 gene
Emerging tests
urinary leukotriene metabolites
Test
Multidrug resistance-associated protein 2 (MRP2) also transports leukotrienes into the bile. When this is defective, there is also increased urinary excretion of leukotriene metabolites. This may become a useful noninvasive test for DJS but is not yet in widespread clinical use.[39]
Result
elevated
Use of this content is subject to our disclaimer