Etiology
Factors such as coughing, retching, vomiting, straining, hiccups, closed-chest pressure or cardiopulmonary resuscitation, acute abdominal blunt trauma, alcohol, medications (aspirin or other nonsteroidal anti-inflammatory drugs), chemotherapeutic agents, and esophageal instrumentation have been associated with MWT.
Hiatus hernia, which is present in 40% to 100% of people with MWT, is considered by many to be a precipitating factor, causing an esophageal tear to occur.[4][15][16] However, in >40% of patients an identifiable risk factor is not found.[14]
Conditions that may induce vomiting include:[12][17][18][19]
Gastrointestinal disease (e.g., food poisoning [particularly when due to Bacillus cereus, vomiting occurs soon after ingestion of contaminated food], infectious gastroenteritis, peptic ulcer disease, malrotation, intussusception, volvulus, gastric outlet obstruction, and gastroparesis)
Hepatobiliary disease (e.g., hepatitis, gallstones, and cholecystitis)
Hyperemesis gravidarum
Renal disease (e.g., urinary tract infection, nephrolithiasis, renal failure, and ureteropelvic obstruction)
Neurologic disease (e.g., tumors, hydrocephalus, congenital disease, trauma, meningitis, pseudotumor cerebri, migraine headaches, and seizures)
Psychiatric disease (e.g., anorexia nervosa, bulimia, and cyclic vomiting syndrome).
Other conditions or agents that may induce vomiting include:[20][21][22]
Toxins
Polyethylene glycol lavage (bowel preparation for colonoscopy)
Chemotherapy agents (e.g., cisplatin)
Postanesthesia or postsurgery.
A chronic cough can be associated with whooping cough, bronchitis, bronchiectasis, emphysema, COPD, or lung cancer.[23]
Pathophysiology
The pathogenesis of MWT is not completely understood. However, most cases seem to occur as a result of a sudden rise in abdominal pressure or transmural pressure gradient across the gastroesophageal junction with a corresponding low intrathoracic pressure. When these forces are high enough to cause distention in this poorly distended area, an acute gastroesophageal tear or laceration may occur.
Classification
Number of lesions
MWT is generally classified by the number of lesions/tears:
Single tear
Multiple tears
Endoscopic classification[2]
Proposed endoscopic classification according to endoscopic features of the tear.
Clean base
Nonbleeding adherent clot
Nonbleeding visible vessel (before or after clot removal)
Actively bleeding or spurting
Esophageal rupture or perforation (Boerhaave syndrome).
The classification allows physicians to provide a prognosis to determine which patients are safe for discharge, and to plan for those who require further treatment.
[Figure caption and citation for the preceding image starts]: Bleeding Mallory Weiss Tear viewed on retroflexionFrom the personal collection of Douglas Adler; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Mallory Weiss tear after application of through-the-scope clip results in hemostasisFrom the personal collection of Douglas Adler; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Mallory Weiss tear after application of through-the-scope clip results in hemostasisFrom the personal collection of Douglas Adler; used with permission [Citation ends].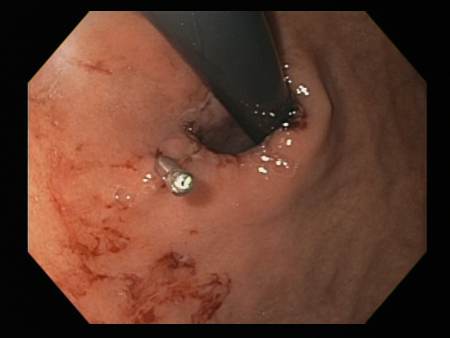
Use of this content is subject to our disclaimer