Approach
The presentation of DN is variable from one patient to another. Up to 50% of patients with DN may be completely asymptomatic.[1][3] Characteristic history and clinical examination findings are often sufficient to diagnose established DN. There are no distinguishing features unique to DN, so all other possible causes of the neuropathy (e.g., hypothyroidism, vitamin B12 deficiency, uraemia, chronic alcoholism) must be ruled out by careful history, physical examination, and laboratory tests. Some of these conditions occur more frequently in people with diabetes and, therefore, may co-exist. For instance, long-term metformin use is associated with vitamin B12 deficiency.[64]
Many of the symptoms associated with diabetic autonomic neuropathy are common in the general population. The symptoms are frequently non-specific, making confirmation of the cause all the more challenging.
Distinguishing diabetic neuropathies from other polyneuropathies
It is important to exclude other causes of peripheral neuropathy that may be erroneously diagnosed secondary to diabetes. A careful history and examination remains the cornerstone of identifying and differentiating other neuropathies presenting in a similar way. Screening laboratory tests should include thyroid function tests, vitamin B12, immunoglobulin electrophoresis, electrolytes, full blood count (FBC), and erythrocyte sedimentation rate (ESR).
An important differential is chronic inflammatory demyelinating polyneuropathy (CIDP). This condition is responsive to immunotherapy and may be more common in patients with diabetes. Patients with CIDP present with tingling, pain, and in particular distal muscle weakness. Nerve conduction studies can specifically identify a reduction in nerve conduction, conduction block, and abnormal temporal dispersion.
History for diabetic peripheral neuropathy
The history may reveal the presence of risk factors strongly associated with DN, including a long duration of diabetes (e.g., >10 years), older age (e.g., >70 years), tall stature, and poorly controlled hyperglycaemia. Intensive blood glucose control is associated with lower rates of DN compared with conventional management.[9][30] History of dyslipidaemia with elevated triglycerides and hypertension may also be present. In addition, a history of recent falls should be elicited, which may reflect gait and balance disorders.[65]
The pain of DN usually presents with sensory symptoms. These begin symmetrically in the toes and slowly advance up to the calves, before beginning in the fingers followed by the arms.[7]
Symptoms vary according to the class of sensory fibres involved. The most common symptoms are induced by the involvement of small fibres and include:[7]
Pain (burning, stinging, shooting, or deep aching)
Dysaesthesias (unpleasant abnormal sensations of burning, tingling, numbness)
Numbness.
Pain is often the reason why patients with DN seek medical care. Intensity varies from mild discomfort to being disabling, and may be described as:
Sticking
Lancinating
Prickling
Burning
Aching
Boring or gnawing
Excessively sensitive.
Pain is often worse at night and may disturb sleep. Involvement of larger fibres may lead patients to complain of a feeling like walking on cotton wool.
The most distal portion of the longest nerves is affected first. Early symptoms typically involve the tips of the toes and fingers. This proceeds proximally, resulting in a 'stocking-glove' pattern of pain and sensory loss. [Figure caption and citation for the preceding image starts]: Progressive axonal loss in diabetic peripheral neuropathyEdwards JL, et al. Pharmacol Ther. 2008 Oct;120(1):1-34; used with permission [Citation ends].
Feeling may also be lost in the feet, with or without pain or dysaesthesias. If nociceptive fibres are involved, loss of sensation may set the stage for painless injuries. An object may become lodged in the shoe and erode through the skin with normal walking and weight-bearing.[Figure caption and citation for the preceding image starts]: Plantar ulcer due to a coin in the shoe of a patient with an insensate footFrom the collection of Dr Rayaz Malik, Weill Cornell Medicine [Citation ends].
Patients presenting with painful DN should be assessed for presence of mood and sleep disorders (e.g., major depressive disorder, obstructive sleep apnoea), as these can impact perception of pain.[66]
Weakness is another presenting symptom but is less common, usually minor, and occurs later in the disease process.
History for diabetic autonomic neuropathy
Symptomatic autonomic neuropathy is infrequent and, in general, occurs later in the course of the disease.[67][68][69]
Patients may have exercise intolerance due to a reduced response in heart rate and blood pressure (BP), and blunted increases in cardiac output in response to exercise.[70]
Orthostatic hypotension, defined as a fall in systolic (20 mmHg) or diastolic (10 mmHg) BP within 3 minutes of standing, occurs in people with diabetes largely as a consequence of efferent sympathetic vasomotor denervation, with reduced vasoconstriction of the splanchnic and other peripheral vascular beds. Symptoms associated with orthostatic hypotension include:
Light-headedness
Weakness
Faintness
Dizziness
Visual impairment
Syncope on standing.
Gastrointestinal (GI) symptoms are relatively common among patients with diabetes and often reflect diabetic GI autonomic neuropathy. Some studies have described the presence of delayed gastric emptying in up to 50% of patients with longstanding diabetes, and in severe cases it is associated with significant impairments in both quality of life and glycaemic control.[71] Although GI symptoms are common in diabetes, symptoms are often due to factors other than autonomic dysfunction. While the delay in gastric emptying is not always clinically apparent, the range of symptoms may include:[72]
Nausea
Post-prandial vomiting
Bloating
Loss of appetite
Early satiety.
Oesophageal dysfunction partly results from vagal dysfunction and may present with symptoms that include heartburn and dysphagia for solids.
Intermittent diarrhoea is evident in 20% of diabetic patients particularly those with known autonomic dysfunction.[67] Profuse watery diarrhoea typically occurs at night, especially in patients with type 1 diabetes. It may alternate with constipation and is extremely difficult to treat. History should rule out other causes of diarrhoea, especially ingestion of lactose, non-absorbable hexitols, or medication.[67]
People with diabetes may also experience faecal incontinence, due to poor sphincter tone.
Bladder dysfunction and impaired ability to void is present in up to 50% of people with diabetes and may result in symptoms of:
Frequency
Urgency
Nocturia
Hesitancy in micturition
Weak stream
Dribbling urinary incontinence
Urine retention.
Erectile dysfunction (ED) is present in 30% to 75% of men with diabetes and can be the earliest symptom of diabetic autonomic neuropathy. However, it is generally accepted that ED is not solely induced by autonomic neuropathy, but rather by the co-existence of other multiple vascular risk factors, such as:
Hypertension
Hyperlipidaemia
Obesity (leading to increased aromatase activity and reduced androgens)
Psychogenic factors.
Women with diabetes may have decreased sexual desire and increased pain during intercourse, and are at risk of decreased sexual arousal and inadequate lubrication.[73]
Sudomotor dysfunction manifests as anhidrosis, heat intolerance, dry skin, or hyperhidrosis.
Hypoglycaemia unawareness may be related to autonomic neuropathy but a study of patients with type 1 diabetes failed to confirm this association.[74]
Other types of DN
Other presentations of DN include:
Mononeuropathies (e.g., carpal tunnel syndrome [median nerve], foot drop [common peroneal nerve])
Cranial neuropathies (extremely rare)
Diabetic truncal radiculoneuropathy (pain over the lower thoracic or abdominal wall)
Diabetic amyotrophy (severe weakness, pain, and proximal thigh muscle atrophy).
Assessment of symptoms
Questionnaires have been developed to investigate orthostatic symptoms and their severity. Current validated autonomic scales include the Autonomic Symptom Profile (ASP) and the Survey of Autonomic Symptoms (SAS).[75][76] The Gastroparesis Cardinal Symptom Index (GCSI) is a reliable and valid instrument, which assesses the severity of patient-reported gastroparesis symptoms.[77]
The effect of pain on patients' function and quality of life may be assessed using scales such as the Brief Pain Inventory Short Form - Diabetic Peripheral Neuropathy (BPI-DPN) and the Norfolk Quality of Life - Diabetic Neuropathy (QOL-DN).[66]
Physical exam
Physical examination (neurological) may reveal symmetrical distal sensory loss, with reduced or absent ankle reflexes. Sensory loss is defined in terms of extent, distribution, and modality and involves assessment of:
Pinprick sensation
Light touch
Vibration
Joint position.
A potentially quick, inexpensive, and accurate screening instrument to evaluate high-risk patients with established DN in the clinic includes assessment for:[78][79]
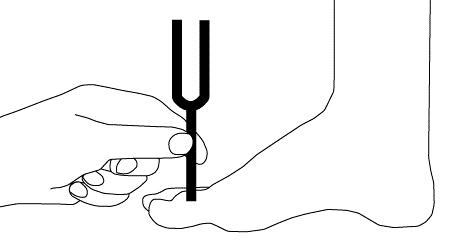
Loss of vibration sense (using a 128-Hz tuning fork) is tested initially at the big toe. Vibration sensation should be tested bilaterally by placing the tuning fork over the dorsum of the big toe, on the bony prominence of the distal interphalangeal (DIP) joint. The patient, whose eyes are closed, should be asked to indicate when he or she can no longer sense the vibration from the vibrating tuning fork. A trial should be conducted when the tuning fork is not vibrating to be certain that the patient is responding to vibration and not pressure. [Figure caption and citation for the preceding image starts]: Vibratory testingCreated by the BMJ Group [Citation ends].
Ankle reflexes offer a quick and inexpensive means to identify high-risk patients in the clinic. Ankle reflexes should be examined using an appropriate reflex hammer (e.g., Tromner or Queen square). Ankle reflexes should be elicited in the sitting position with the foot dependent and the patient relaxed. In addition, the foot should be passively positioned and slightly dorsiflexed to obtain optimal stretch of the muscle. The Achilles tendon should be percussed directly. If the reflex is obtained, it is graded as present. If the reflex is absent, the patient should be asked to perform the Jendrassic manoeuvre (i.e., hooking the fingers together and pulling). Reflexes elicited with the Jendrassic manoeuvre are designated as present with reinforcement. If the reflex is absent, even with the Jendrassic manoeuvre, the reflex is considered absent.
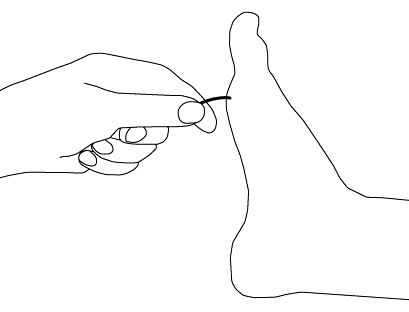
Loss of light touch (using 10-g monofilament) is tested at the dorsal aspects of both big toes. For this examination, it is important that the patient's foot be supported (i.e., allowing the sole of the foot to rest on a flat, warm surface). The filament should initially be pre-stressed (4-6 perpendicular applications to the dorsum of the examiner's first finger). The filament is then applied to the dorsum of the big toe midway between the nail fold and the DIP joint. The toe should not be held directly. The filament is applied perpendicularly and briefly (<1 second), with an even pressure. When the filament bends, the force of 10 g has been applied. The patient, whose eyes are closed, should be asked to respond 'yes' if he or she feels the filament. Eight correct responses out of 10 applications is considered normal; 1-7 correct responses indicates reduced sensation; no correct answers translates into absent sensation. [Figure caption and citation for the preceding image starts]: Light touch testing with monofilamentCreated by the BMJ Group [Citation ends].
Presence of ulcers, callus, and prior amputations (foot inspection).
Painless injuries may be apparent on exam. These often occur over pressure points on the foot and most commonly over the metatarsal heads. Infection often complicates the situation and can be followed by gangrene if vascular dysfunction is present.[Figure caption and citation for the preceding image starts]: Plantar ulcer in a patient with type 1 diabetesFrom the collection of Dr Rodica Pop-Busui, University of Michigan [Citation ends].
In patients with involvement of large sensory fibres, gait ataxia may develop, especially at night or when the patient walks with closed eyes. In patients with severe DN, motor involvement may become clinically apparent with weakness of toe dorsiflexion and intrinsic hand muscles.
Resting tachycardia and a fixed heart rate are characteristic late findings in diabetic patients with vagal impairment. Resting heart rates of 90-100 bpm and occasional heart rate increments up to 130 bpm occur.[70] Resting heart rate and heart rate variation (HRV) are easy to measure at the bedside, and can reveal early signs of cardiac autonomic neuropathy (CAN). However, resting tachycardia is not a specific sign of CAN.
Measurement of supine and standing BP is important to diagnose orthostatic hypotension. Orthostatic hypotension may be present in advanced CAN but requires prior exclusion of other causes and is an insensitive index. QTi prolongation and reverse dipping on ambulatory BP monitoring are specific but insensitive indices of CAN.[23][80]
Bladder dysfunction may ultimately result in urinary retention with evidence of an enlarged bladder on abdominal examination.
Investigations
DN is often a clinical diagnosis. There are differences between diagnostic criteria for clinical care and clinical research.[3][23] It is recommended that the diagnosis and classification of DN for research and clinical trials be based on at least one standardised measure from each of the following categories:[3][81][82]
Clinical symptoms
Clinical examination
Basic laboratory tests
Electrophysiological testing
Quantitative sensory testing (QST)
Autonomic testing
Skin biopsy or non-invasive technique (e.g., corneal confocal microscopy) to assess nerve fibres.
Basic laboratory tests include fasting blood glucose, HbA1c, and plasma glucose measured 2 hours after 75 g oral glucose load, thyroid-stimulating hormone, vitamin B12, serum urea, immunoglobulin electrophoresis, and ESR.
Skin biopsy is a validated technique for determining intra-epidermal nerve fibre density, and may be considered for the diagnosis of DN, particularly small-fibre neuropathy.[82] Newer non-invasive modalities such as corneal confocal microscopy (CCM), a technique used to image the corneal sub-basal nerve plexus, and laser Doppler imaging flare technique (LDI flare), which assesses the small-fibre axon reflex-mediated neurogenic vasodilatory response to cutaneous heating, have been shown to be comparable to intra-epidermal nerve fibre density.[83][84]
Electrophysiological testing (nerve conduction tests and electromyography [EMG]) and specialised neurology evaluation are needed in situations where the clinical features are atypical (e.g., where motor deficits exceed sensory deficits; marked asymmetry of the neurological deficits; initial symptoms in the upper extremities; rapid progression).[Figure caption and citation for the preceding image starts]: Nerve conduction testing of the lower legCreated by the BMJ Group [Citation ends].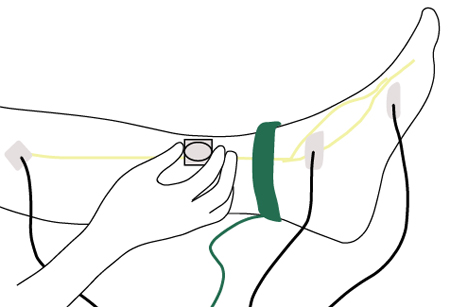
QST quantifies vibration perception threshold (VPT) and thermal perception threshold. A variety of instruments, using a variety of algorithms, facilitate sensory threshold determination. Two general schemes have emerged: the method of limits and the method of levels. In the method of limits, a patient is required to indicate as soon as they detect an increasingly strong stimulus (ascending ramp) or when they no longer detect a decreasing stimulus (descending ramp). In the method of levels, stimuli of defined intensity levels are tested with the patient indicating whether they detect a specific level; the patient is forced to choose whether they feel a stimulus. Therefore, the method of levels is also referred to as a forced-choice algorithm.[85] QST can be used when the rest of the examinations are normal, to detect small-fibre neuropathy.[86] An assessment of autonomic neuropathy relies principally on cardiovascular autonomic function testing, which can be complex to perform. CCM has been shown to have an extremely high sensitivity and specificity for diabetic autonomic neuropathy.[87]
Cardiovascular autonomic reflex tests (CARTs)[23][68][69][88]
CARTs should be performed using a battery of validated tests (e.g., respiratory rate [RR] response to deep breathing, Valsalva manoeuvre, and RR response to postural changes), rather than one single test. These provide information mainly on parasympathetic function, whereas the BP response to standing and to Valsalva manoeuvre, and the sustained isometric muscular strain, may provide information on sympathetic function.
The RR response to deep breathing is the most widely used test of cardiovagal function, with approximately 80% specificity.
The Valsalva manoeuvre needs greater co-operation from patients and cannot be universally performed. Heart rate (HR) response depends on the BP response to the manoeuvre; the BP response to sustained handgrip is no longer regarded as an established clinical test but only as an investigational test. The orthostatic hypotension test may still be used in the standard assessment of CAN, despite its low sensitivity.[23]
These tests are non-invasive, safe, clinically relevant (they correlate with tests of peripheral nervous system function), easy to perform, sensitive, specific, reproducible, and standardised, and, therefore, they are considered consolidated, preferred standard measures of autonomic function. For the diagnosis and monitoring of CAN, more than one CART and BP test are required.
Heart rate variability (HRV)[68][69]
HRV can be assessed either by calculating indices based on statistical analysis of response rate intervals (time-domain analysis) or by spectral analysis (frequency-domain analysis) of an array.[70]
Time-domain indices of global HRV and total spectral power of HRV represent an index of parasympathetic activity, as well as the HRV spectral power in the high frequency region, while the low frequency relative proportion (not the absolute power) of HRV provides a relative measure of sympathetic modulation. This interpretation should be made with caution if respiratory artifacts (slow breaths) cannot be excluded.[88]
It is generally accepted that, at this time, the use of HRV should be reserved for clinical research studies.
QT prolongation is an independent predictor of mortality in diabetic patients and is weakly associated with measures of HRV.[89]
Age-related normal ranges of HR tests are strictly required.
Presence of CAN, as assessed by impaired HRV, is an important independent predictor of all-cause and cardiovascular mortality.[23][68][69]
The following investigations are performed only if the history and physical examination reveal concerns about the possibility of any of these specific autonomic manifestations.
Gastric emptying studies with double-isotope scintigraphy detect abnormalities in GI pacemaking. This may help in the diagnosis of gastroparesis where the diagnosis is in doubt.
Hydrogen breath tests using non-radioactive 13C-acetate or -octanoic acid as a label are safe, inexpensive, and correlate well with scintigraphy results.
A barium meal investigation has a place in evaluating mucosal lesions or obstruction.
Gastroduodenoscopy is also recommended to exclude pyloric or other mechanical obstructions.
Two-dimensional gastric ultrasonography has been validated for measuring emptying of liquids and semi-solids. However, three-dimensional ultrasound offers a more comprehensive imaging of the total stomach.
Anorectal manometry is indicated for evaluating sphincter tone and the rectal-anal-inhibitory reflex. It can distinguish colonic hypomotility from rectosigmoid dysfunction causing outlet obstructive symptoms.
For large-volume diarrhoea, faecal fat should be checked and further studied with a 72-hour faecal fat collection and/or the d-xylose test to rule out malabsorptive disorders. If there is significant steatorrhoea, pancreatic function tests should be performed. If coeliac disease is suspected (increased risk in type 1 diabetes), serum levels of coeliac disease antibody profile, including anti-transglutaminase and anti-endomysial antibodies, should be measured.
Patients with ED should be investigated with a morning serum total testosterone.[39][90] Further specialised testing may also be necessary. See Erectile dysfunction.
Diabetic bladder dysfunction should be evaluated by:[91]
Urinary culture
Post-void ultrasound, to assess residual volume and upper-urinary tract dilation
Cystometry and voiding cystometrogram
Video-urodynamic studies.
Investigations for suspected infection/osteomyelitis
Inflammatory serum biomarkers such as C-reactive protein (CRP), ESR, or procalcitonin should be assessed when there is a possible infected foot ulcer, particularly when the clinical examination is diagnostically equivocal or uninterpretable. Magnetic resonance imaging has emerged as the most accurate means of diagnosing osteomyelitis and should be used when there is doubt about the diagnosis despite clinical, plain x-rays, and laboratory findings. Bone biopsy for culture and histopathology can also aid with diagnosis and management.[92][93]
Further investigations mainly used in research
GI neuropathies
GI manometry should be considered as a research technique to investigate gastric and intestinal motility/emptying.
Gastric MRI has been used to measure gastric emptying and motility with excellent reproducibility, but its use is limited to research purposes.
Assessment of sudomotor innervation
Used mainly for research due to limited data.
Tests of sudomotor function evaluate the extent, distribution, and location of deficits in sympathetic cholinergic function. These tests may include:
Quantitative sudomotor axon reflex test (QSART)
Sweat imprint
Thermoregulatory sweat test (TST)
Sympathetic skin response: some devices can provide a quantitative assessment of sudomotor function using direct current stimulation and reverse iontophoresis. These devices measure the ability of sweat glands to release chloride ions in response to electrochemical activation by recording local skin conductance.[67][68][69][94]
Quantitative scintigraphic assessment of sympathetic innervation of the human heart is possible using single photon emission computed tomography (SPECT) with 123I-meta-iodobenzylguanidine (MIBG) and positron emission tomography (PET) with 11C-meta-hydroxyephedrine.[95] However, no standardised methods or normative values exist, and the high costs and the available data on the reproducibility limit their use to research only.[68][69]
Sympathetic outflow, at rest and in response to various physiological perturbations, can be measured directly by microelectrodes inserted into a fascicle of a distal sympathetic nerve to the skin or muscle (muscle sympathetic nerve activity). This is also used for research purposes only.[68][69][88]
Cardiac vagal baroreflex sensitivity may also be used in research protocols to assess cardiac vagal and sympathetic baroreflex function.
Additional research investigations include 24-hour BP profile and microneurography. Attenuation (non-dipping) and loss of BP nocturnal fall (reverse dipping) on ambulatory BP monitoring have been associated with cardiovascular autonomic neuropathy and attributed to disruption of circadian variation in sympathovagal activity.[96] In diabetic patients non-dipping or reverse dipping are independent predictors of cardiovascular events and the progression of diabetic nephropathy. Microneurography is based on recording electrical activity emitted by peroneal, tibial, or radial muscle sympathetic nerves and identifying sympathetic bursts. Fully automated sympathetic neurogram techniques provide a rapid and objective method that is minimally affected by signal quality and preserves beat-by-beat sympathetic neurograms.[68][69][88][97]
Pain-related evoked potentials
Used for research only.
Nerve axon reflex/flare response
Stimulation of the nociceptive C fibre results in both orthodromic conduction to the spinal cord and antidromic conduction to other axon branches, which stimulates the release of peptides, such as substance P and calcitonin gene related peptide, which causes vasodilation and increased blood flow. This is known as the axon reflex or flare response. An impaired axon reflex indicates small-fibre neuropathy.
Used for research only. More data are needed before this test can be recommended for clinical use.[98]
Neuropad
A simple visual indicator test, which uses a colour change to define the integrity of the skin sympathetic cholinergic innervation.
Neuropad responses have been shown to correlate with the modified neuropathy disability score (NDS), QST, and intra-epidermal nerve fibre (IENF) loss with relatively high sensitivity, but lower specificity for detecting distal symmetrical polyneuropathy (DSPN).[99]
However, the studies had relatively small samples and, therefore, this test requires further validation.
Assessment for common comorbidities
Diabetes-related foot disease
DN is the primary cause of diabetic foot problems and ulceration, the leading causes of diabetes-related hospital admissions and non-traumatic amputation.[4]
The diagnosis of foot complications in a person with diabetes is a clinical diagnosis based on thorough history and examination.
Retinopathy
All patients with diabetes are regularly screened for retinopathy.
Signs of retinopathy include decreased vision, retinal findings including dot and blot haemorrhages, microaneurysms (background retinopathy), and/or neovascularisation (proliferative retinopathy).
See Diabetic retinopathy.
Nephropathy
All patients with diabetes receive regular monitoring of renal function. Evaluation should include urea, creatinine, urinary albumin to creatinine ratio (ACR), and measurement of estimated glomerular filtration rate.
Patients are often asymptomatic and may not develop symptoms until advanced stages of nephropathy. In advanced stages, initial constitutional symptoms may be non-specific (e.g., fatigue and anorexia).
Presence of other microvascular complications of diabetes (neuropathy, retinopathy) should prompt evaluation for diabetic kidney disease.
Peripheral arterial disease
Peripheral arterial disease may be missed in patients with DN, as perception of rest pain and claudication is reduced.
Ankle-brachial index (ABI) may be unreliable in patients with diabetes; other tests such as toe-brachial index may be considered for diagnosis.[100]
Depression
Diabetic peripheral neuropathy is associated with comorbid mood disorders, particularly depression and anxiety.[24][66][101][102] The presence of mood disorders can affect perception of pain.
Presence of depressive symptoms appears to be influenced by pain, perceptions of DN symptom unpredictability, the lack of treatment control, restrictions in activities of daily living, and changes in social self-perception.[24][103]
Screening with a validated tool such as the Patient Health Questionnaire (PHQ)-9 may help with identification and diagnosis.
Sleep disorders
Use of this content is subject to our disclaimer