Case history
Case history #1
A 63-year-old woman with diabetes presents with an episode of retrosternal chest pain and diaphoresis that occurred while walking upstairs earlier that day. Her examination is unremarkable except for blood pressure 156/96 mmHg and abdominal obesity. A recent lipid profile showed triglyceride 3.8 mmol/L (335 mg/dL), total cholesterol 6.29 mmol/L (243 mg/dL), low-density lipoprotein cholesterol 3.68 mmol/L (142 mg/dL), and high-density lipoprotein cholesterol 0.88 mmol/L (34 mg/dL). Her electrocardiogram shows no acute changes.
Case history #2
A 56-year-old obese man with poorly controlled type 2 diabetes mellitus presents with symptoms of nausea, vomiting, and worsening abdominal pain after a dinner of steak, chips, and wine. On examination he has diffuse abdominal tenderness, which is most marked in the left upper quadrant. Eruptive xanthomas are noted on his back and forearms. His triglyceride level is 28.3 mmol/L (2500 mg/dL) and his blood glucose is 20.2 mmol/L (364 mg/dL). Serum lipase levels are elevated and abdominal ultrasound shows evidence of pancreatitis.
Other presentations
HTG is typically clinically silent and is usually detected by lipid screening.[5] Presence of physical findings in severe HTG is becoming less common, likely due to earlier diagnosis and more effective treatment.[12] There are no symptoms or physical findings in patients with mild-to-moderate HTG, unless atherosclerotic cardiovascular disease has developed, which can lead to symptoms of acute coronary syndromes. However, some secondary factors underlying HTG, such as type 2 diabetes mellitus, metabolic dysfunction-associated steatotic liver disease (previously known as non-alcoholic fatty liver disease), renal disease, or hypothyroidism, are themselves associated with specific clinical features.[4][13]
Characteristic clinical features of chylomicronaemia include eruptive xanthomas, lipaemia retinalis, hepatosplenomegaly, abdominal pain, and nausea and vomiting.[14] Less common clinical features include intestinal bleeding, pallor, anaemia, irritability, diarrhoea, seizures, and encephalopathy.[14] Infants with familial chylomicronaemia syndrome can present with failure to thrive and abdominal pain.[14]
[Figure caption and citation for the preceding image starts]: Eruptive xanthomasFrom the personal collection of Professor Hegele; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Lipaemia retinalis. Pinkish-white discolouration of retinal blood vessels on ophthalmoscopyFrom the personal collection of Professor Hegele, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Lipaemia retinalis. Pinkish-white discolouration of retinal blood vessels on ophthalmoscopyFrom the personal collection of Professor Hegele, used with permission [Citation ends].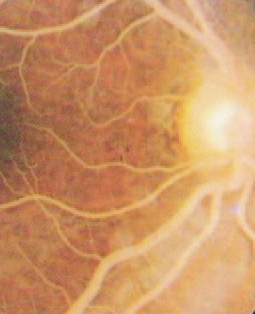
Use of this content is subject to our disclaimer