Aetiology
Meconium is the first stool of the newborn. It is a collection of secretions from the fetal intestine and is a sterile, thick, black-green, viscous material containing pancreatic and biliary secretions, swallowed fetal cells, hair, and vernix. If aspirated into the lungs it causes local inflammation of the airways and release of several cytokines.
Presence of meconium in the amniotic fluid and aspiration of meconium-stained amniotic fluid (MSAF) are the main causes of MAS. Passage of meconium may be a physiological maturation phenomenon during fetal development, and MSAF is uncommon between 20 weeks' and 34 weeks' gestation.[18] During delivery, between 2% and 9% of neonates with meconium passage aspirate the meconium, triggering lung injury and respiratory distress.[6]
MSAF may have pathological causes: fetal distress and intrapartum hypoxia secondary to placental insufficiency, cord compression, cord around the neck, oligohydramnios, maternal hypertension, pre-eclampsia, maternal diabetes, maternal drug abuse, or smoking.[19] These factors can lead to gasping and aspiration of meconium by the fetus and the newborn. Puerperal infection (chorioamnionitis and endometritis) is also associated with MSAF.[20] This may be due to fetal stress and passage of meconium.
Pathophysiology
The pathophysiology of MAS can be explained on the basis of mechanical, vascular, metabolic, and inflammatory effects of meconium.[21][22] Although meconium may be passed spontaneously, intrauterine hypoxia may trigger passage of fresh meconium and fetal gasping. This leads to aspiration of amniotic fluid containing the meconium.
The aspirated meconium may cause partial or total airway obstruction depending on the consistency of the fluid. Diffusion of particulate material causes lower airway obstruction, leading to complete atelectasis, or incomplete airway blockage with a ball-valve obstruction. This phenomenon results in air trapping with eventual pneumothorax or pneumomediastinum. Atelectasis leads to right-to-left shunting of blood without oxygenation at the alveolar level. Air trapping from a ball-valve obstruction causes accumulation of carbon dioxide. Together they produce severe hypoxia, hypercarbia, and acidosis. Both hypoxia and acidosis are potent pulmonary vasoconstrictors that result in further right-to-left shunting. The combination of non-uniform atelectasis and pulmonary vasoconstriction can lead to mismatching of ventilation and perfusion (V/Q abnormalities).
In addition, meconium also causes an inflammatory reaction in the alveoli and larger airways, which triggers generation of various inflammatory cytokines.[23] Meconium itself may cause local inflammation of the airways and inactivation of surfactant, which leads to alveolar atelectasis.[24] Vasoactive mediators play a major role in the development of persistent pulmonary hypertension of the neonate in MAS, and prolonged hypoxia in utero also causes hypertrophy of pulmonary vascular bed (remodelling), leading to pulmonary hypertension.[25][Figure caption and citation for the preceding image starts]: Cross-section of lung at autopsy showing massive amount of meconium in the airwaysFrom the personal collection of Dr Vidyasagar and Dr Bhat [Citation ends].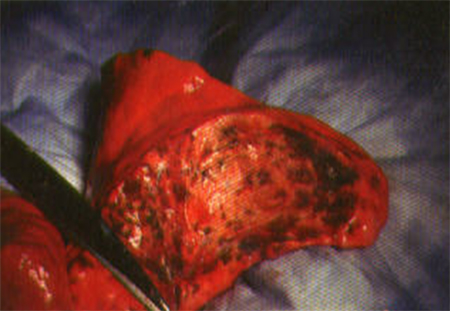 [Figure caption and citation for the preceding image starts]: Air trappingFrom the personal collection of Dr Vidyasagar and Dr Bhat [Citation ends].
[Figure caption and citation for the preceding image starts]: Air trappingFrom the personal collection of Dr Vidyasagar and Dr Bhat [Citation ends].
[Figure caption and citation for the preceding image starts]: Pathophysiology of meconium aspiration syndromeCreated by Dr Vidyasagar and Dr Bhat [Citation ends].
Use of this content is subject to our disclaimer