Etiology
There are many causes of hemolysis.
Hereditary causes fall into three broad categories:[1][2]
Inherited red blood cell (RBC) defects (membrane defects) - hereditary spherocytosis, elliptocytosis, pyropoikilocytosis
Enzyme deficiencies - glucose-6-phosphate dehydrogenase deficiency, pyruvate kinase deficiency
Abnormal Hb production - sickle cell anemia, thalassemia.
Acquired hemolytic anemia can be subdivided into immune and nonimmune etiologies:
Autoantibodies - the cause of immune-mediated hemolytic anemias, most often as part of other autoimmune conditions (e.g., systemic lupus erythematosus, rheumatoid arthritis, scleroderma) or related to a lymphoproliferative disorder (non-Hodgkin lymphoma, chronic lymphocytic leukemia).
Immune hemolytic anemias - divided into warm- or cold-reacting antibodies, depending on the temperature at which the antibody binds most avidly to the RBCs.
Alloimmune hemolytic anemias - include hemolytic disease of the newborn or transfusion reaction.
Drugs - some through immune-mediated mechanisms and others through nonimmune-mediated mechanisms.
Other nonimmune-mediated causes - include infection, trauma in various forms (microangiopathic hemolysis such as disseminated intravascular coagulation, thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, malignant hypertension, eclampsia, HELLP syndrome [hemolysis, elevated liver enzymes, low platelet count] in pregnancy, mechanical prosthetic heart valves, march hemolysis, thermal injury, osmotic lysis), hypersplenism, and liver disease.
Paroxysmal nocturnal hemoglobinuria - a rare disorder resulting in an acquired RBC membrane defect and subsequent hemolysis.
Pathophysiology
Hemolytic anemia results from either intravascular or extravascular red blood cell (RBC) destruction.
Extravascular hemolysis results from accelerated red cell destruction by cells of the reticuloendothelial system, due to immune targeting by antibodies, as occurs in a warm autoimmune hemolytic anemia. Intravascular hemolysis results from red cell destruction within the vasculature, due to complement-mediated lysis or direct red cell trauma from a prosthetic heart valve or microangiopathic process.
Autoimmune hemolysis is most often due to extravascular destruction of red cells coated with an autoantibody (positive direct antiglobulin test [Coombs positive]). Because sections of the RBC membrane are removed by the reticuloendothelial cells, RBCs with a smaller surface area appear as spherocytes on the peripheral smear. In contrast, traumatic disruption of red cells by microangiopathic processes results in the production of red cell fragments, or schistocytes, on the smear. This also results in the release of RBC lactate dehydrogenase and hemoglobin (Hb) into the circulation, which can result in hemoglobinuria. Free Hb is bound by haptoglobin, resulting in the decrease in haptoglobin that is observed in many cases of hemolytic anemia.
Hereditary causes of hemolytic anemia, including membrane defects, enzyme mutations, and hemoglobinopathies, generally result in anemia due to significantly shortened RBC lifespan and removal of senescent red cells by the spleen. [Figure caption and citation for the preceding image starts]: Peripheral blood smear with spherocytes, reticulocytes, and a nucleated red blood cellFrom the collection of John Densmore, Department of Medicine, University of Virginia [Citation ends].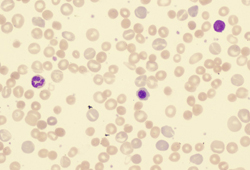 [Figure caption and citation for the preceding image starts]: Peripheral blood smear with red blood cell fragments, or schistocytes (arrow)From the collection of John Densmore, Department of Medicine, University of Virginia [Citation ends].
[Figure caption and citation for the preceding image starts]: Peripheral blood smear with red blood cell fragments, or schistocytes (arrow)From the collection of John Densmore, Department of Medicine, University of Virginia [Citation ends].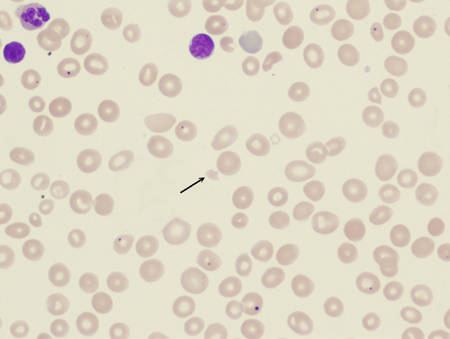
Classification
Acquired hemolytic anemia: immune or nonimmune
Immune (direct antiglobulin test often positive):
Warm antibody autoimmune hemolytic anemia: antibody (usually IgG) binds most avidly at core body temperature. Associated with underlying diseases such as systemic lupus erythematosus, lymphoma, and chronic lymphocytic leukemia.
Cold antibody autoimmune hemolytic anemia: antibody binds red blood cell at temperature below body temperature (often IgM, but may be IgG). Can be idiopathic, or associated with infection or malignancy.
Drug-induced immune hemolytic anemia.
Alloimmune hemolytic anemia: hemolytic disease of the newborn or transfusion reaction.
Nonimmune (direct antiglobulin test negative):
Infection: malaria, babesiosis, bartonellosis.
Bacterial toxins: Clostridium perfringens infection.
Drug-induced (by nonimmune mechanism).
Trauma: microangiopathic hemolysis such as disseminated intravascular coagulation, thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, eclampsia, HELLP syndrome (hemolysis, elevated liver enzymes, low platelet count) in pregnancy; mechanical prosthetic heart valve; march hemolysis.
Membrane disorder (acquired): paroxysmal nocturnal hemoglobinuria, liver disease.
Thermal injury.
Osmotic lysis.
Hypersplenism.
Congenital hemolytic anemia[1][2]
Red cell membrane disorders:
Hereditary spherocytosis
Elliptocytosis
Pyropoikilocytosis
Red cell enzyme defects:
Glucose-6-phosphate dehydrogenase deficiency
Pyruvate kinase deficiency
Hemoglobinopathies:
Sickle cell anemia
Thalassemia
Use of this content is subject to our disclaimer