History and exam
Key diagnostic factors
common
history of unprotected intercourse
Chancroid spreads through unprotected intercourse with an infected partner.
history of multiple sex partners
Studies have shown that the minimum number of partners to maintain chancroid in a population is 15 to 20 per year.[11] In most epidemics, commercial sex workers have been an important reservoir.
genital ulcers
Ulcers are soft and painful without induration. They may be painless in women, especially if they occur on the vaginal walls or cervix.
Genital ulcers measure 1-2 cm and have sharply demarcated borders, ragged, undermined edges, and a friable base covered with a grayish or yellow exudate. [Figure caption and citation for the preceding image starts]: Penile ulcers associated with chancroidAdapted from J. Miller, Public Health Image Library, CDC (1974) [Citation ends]. In men, the majority are located on the prepuce or frenulum, or in the coronal sulcus. In women, ulcers are usually on the fourchette, labia, vestibule, or clitoris.
In men, the majority are located on the prepuce or frenulum, or in the coronal sulcus. In women, ulcers are usually on the fourchette, labia, vestibule, or clitoris.
Variant appearances include giant (>2 cm) or serpiginous ulcers, follicular ulcers, papules with a raised border (resembling condyloma latum of secondary syphilis), or lesions <1 to 5 mm in diameter, resembling HSV lesions.[Figure caption and citation for the preceding image starts]: Chancroid pustule resembling syphilisAdapted from Public Health Image Library, CDC (1971) [Citation ends].
inguinal lymphadenitis and buboes
Seen in up to 50% of patients, mostly in men.[52] May be unilateral in approximately two-thirds of cases.
Fluctuant suppurative lymphadenitis (bubo) forms in later stages. [Figure caption and citation for the preceding image starts]: Buboes associated with Haemophilus ducreyi infectionAdapted from S. Lindsley, Public Health Image Library, CDC (1971) [Citation ends].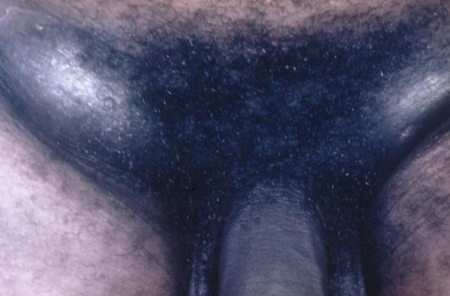
Other diagnostic factors
uncommon
dysuria
May be present in women in some cases.
vaginal discharge
May be present in women in some cases.
dyspareunia
May be present in women in some cases.
rectal pain or bleeding
May be present in women in some cases. Can be due to a fistula or to rectal ulcerations.
rectovaginal fistula
A complication of chancroid. May be present in women in some cases.
urethral fistula
A complication of chancroid. May be present in some cases.
Risk factors
strong
multiple sex partners
Chancroid is not sustainable within a population with low numbers of sex partners. The minimum number of partners to maintain chancroid in a population is 15 to 20 per year.[11]
The exact rate of transmission per sexual act is thought to be high but is not known. The probability of transmission from a single exposure has been estimated to be 0.35.[15]
sexual contact with sex worker
Haemophilus ducreyi has a brief duration of infectivity and requires a frequent turnover of sex partners to be maintained within a population.[11][29][32]
In most epidemics, commercial sex workers have been an important reservoir.
Sex workers have a high number of partners and limited access to health care. Additionally, ulcers in the vagina and on the cervix may be painless and therefore go untreated.[15]
unprotected intercourse
Multiple studies have demonstrated the importance of condom use in reducing the spread of genital ulcerative disease. In Thailand, the 100% condom use policy has been very effective; no cases of chancroid have been seen since 1998. In African countries with higher use of condoms, rates are much lower.[11]
substance abuse
male sex
The incidence of disease is 25:1 (male to female ratio) in outbreaks of chancroid and 3:1 in endemic areas.[17]
There is no sex difference in the formation of papules but women are more likely to have spontaneous resolution of the papule, whereas men are more likely to progress to the pustular stage. The reason for the sex difference is unknown.[35]
Use of this content is subject to our disclaimer