Differentials
Common
Sinus tachycardia
History
history often vague; palpitations that just seem to fade away; hyperthyroidism-associated symptoms such as decreased weight despite increased appetite, emotional lability, oligomenorrhea; associated breathlessness and fatigue due to anemia; can be experienced in the setting of intense emotional episodes; associated headaches and flushing might be due to a pheochromocytoma
Exam
regular pulse >100 bpm; normal cardiac exam; signs and symptoms of hyperthyroidism (e.g., fine tremor, tachycardia, lid lag), anemia (e.g., pallor) or pheochromocytoma (episodic hypertension)
1st investigation
- 12-lead ECG:
regular QRS complexes at a rate of >100 bpm
Other investigations
- thyroid stimulating hormone:
decreased in most cases of hyperthyroidism
- CBC:
decreased Hb if anemia
- pregnancy test:
positive in pregnancy
Atrial tachycardia
History
history of structural heart disease; association with acute illness; palpitations are often paroxysmal; fast and regular palpitations with sudden onset and termination; less specific symptoms such as fatigue and breathlessness can be present if atrial tachycardia is incessant
Exam
often normal; can see signs and symptoms of heart failure or pulmonary disease such as COPD or pneumonia
1st investigation
- baseline ECG without symptoms:
often normal; may see signs of left (biphasic P wave in lead V1 or double-humped P wave in lead II) or right (P wave >2.5 mV in lead II) atrial abnormalities
Other investigations
- ambulatory ECG or event monitor with symptoms:
narrow QRS tachycardia (>100 bpm); P wave sometimes with a non-sinus morphology
Atrial flutter
History
fast and regular palpitations; seen in patients with normal hearts but is more often seen in patients with left ventricular dysfunction or rheumatic heart disease; commonly seen in conjunction with atrial fibrillation
Exam
fluttering of the venous jugular pulse may be seen; arterial pulse typically normal in intensity but ventricular rate is variable depending on the degree of AV block; signs of congestive heart failure and left ventricular dysfunction may be present
1st investigation
- baseline ECG without symptoms:
normal but may see signs of left (biphasic P wave in lead V1 or double-humped P wave in lead II) or right (P wave >2.5 mV in lead II) atrial abnormalities
Other investigations
- ambulatory ECG or event monitor with symptoms:
rapid regular saw-tooth flutter waves at 300 bpm with a narrow complex QRS at some multiple of 300, that is, 150, 100, or 75 bpm
Atrial fibrillation
History
history of congestive heart failure, valvular heart disease, hypertrophic/dilated cardiomyopathy, pericarditis, thyroid disease, pulmonary disease (including asthma), obstructive sleep apnea, or atrial flutter; paroxysmal or persistent palpitations; often associated with other symptoms such as dyspnea or fatigue; or can occur after binge drinking (holiday heart); common in older people; use of omega-3-acid ethyl esters in patients treated for hypertriglyceridemia; may be a history of athletic training
Exam
irregularly irregular pulse; often rapid; if the patient is in a normal rhythm at the time of examination signs of congestive heart failure, rheumatic heart disease, or thyroid disease should be sought
1st investigation
- baseline ECG without symptoms:
normal but may see signs of left (biphasic P wave in lead V1 or double-humped P wave in lead II) or right (P wave >2.5 mV in lead II) atrial abnormalities
Other investigations
- ambulatory ECG or event monitor with symptoms:
irregularly irregular rhythm without discrete P waves
- thyroid stimulating hormone:
may be elevated or decreased
- echocardiogram:
may show left atrial enlargement, mitral regurgitation, left ventricular dysfunction
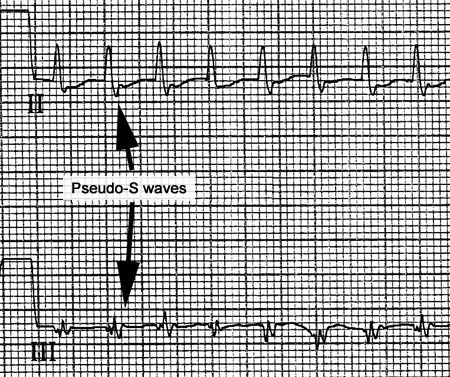
Atrioventricular nodal reentrant tachycardia
History
can occur at any age; symptom onset most common in the late 20s or early 30s; more common in women; palpitations typically have an abrupt initiation and termination, are fast and regular, described as being machine-like, and can be accompanied by a fullness in the throat due to right atrial contractions against a closed tricuspid valve; often terminated with Valsalva maneuvers and sometimes associated with presyncope
Exam
typically normal; during arrhythmia, the pulse is rapid and regular with a rapid fluttering of the jugular venous wave pulse
1st investigation
- baseline ECG without symptoms:
normal
Other investigations
- ambulatory ECG or event monitor with symptoms:
narrow QRS tachycardia, sometimes with pseudo R' in lead V1 or the S wave in the inferior leads
More
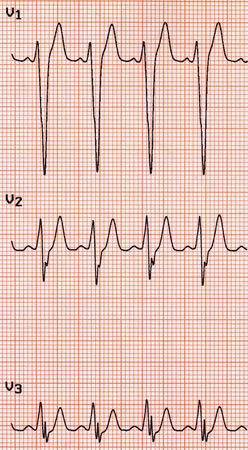
Wolff-Parkinson-White syndrome (WPW)
History
rapid and regular palpitations that can be terminated with Valsalva maneuvers; typically present in the teenage years; more frequently seen in males; associated with a slight increase in incidence of sudden cardiac death
Exam
typically normal at baseline; during palpitations there is a rapid pulse that is regular, except in the case of atrial fibrillation in the setting of WPW, in which case the pulse is irregular
1st investigation
- baseline ECG without symptoms:
evidence of preexcitation with a short PR segment (<120 ms) and delta waves; patients can have WPW with a concealed bypass tract that only conducts as the retrograde limb of the tachycardia circuit, and is not seen on the baseline ECG
More
Other investigations
- ambulatory ECG or event monitor with symptoms:
narrow or wide QRS with ectopic P waves; if atrial fibrillation is present, the ECG can be extremely fast (>200 bpm) with an irregular and wide QRS
Premature ventricular beat
History
usually seen in normal hearts; palpitations are described as an early beat with a pause followed by an unusually strong or "pounding" beat, or simply as a "flip-flop"; may be associated with caffeine intake
Exam
typically normal; peripheral arterial pulse is regular except for occasional premature beats, often with a brief pause afterward
1st investigation
- baseline ECG without symptoms:
typically normal
Other investigations
- ambulatory ECG or event monitor with symptoms:
isolated wide QRS complexes
- echocardiogram:
usually normal
Premature atrial beat
History
usually seen in normal hearts; palpitations described as a skipped beat often with a pause afterward or a brief flip-flop, may be associated with caffeine intake; symptoms are usually not as intense as premature ventricular beats
Exam
typically normal; peripheral arterial pulse is regular except for occasional premature beats, often with a brief pause afterward
1st investigation
- baseline ECG without symptoms:
normal
Other investigations
- ambulatory ECG or event monitor with symptoms:
regular sinus rhythm with occasional premature P waves, sometimes with a morphology different from the sinus P wave
- echocardiogram:
usually normal
Anxiety and panic disorder
History
palpitations may be preceded by a stressful event; tingling, paresthesia, breathlessness may accompany the palpitations
Exam
physical exam is nonspecific
1st investigation
- baseline ECG without symptoms:
normal or sinus tachycardia
Other investigations
- ambulatory ECG or event monitor with symptoms:
normal or sinus tachycardia
Fever
History
sweating, flushing, underlying illness, for example, influenza
Exam
elevated temperature
1st investigation
- none:
diagnosis is based on clinical evaluation
Other investigations
Hyperthyroidism
History
decreased weight despite increased appetite, emotional lability, oligomenorrhea, heat intolerance
Exam
weight loss, hyperreflexia, tachycardia, atrial fibrillation, fine tremor, may be goiter
1st investigation
- ECG:
normal, tachycardia, or evidence of atrial fibrillation
- TFTs:
elevated free T4 and T3, low thyroid stimulating hormone
Other investigations
Excess alcohol use (binge drinking)
History
significant alcohol intake, especially history of binge drinking
Exam
atrial fibrillation may be evident, signs of alcohol intoxication
1st investigation
- none:
diagnosis is based on clinical evaluation
Other investigations
- ECG:
if suspect atrial fibrillation clinically
Caffeine
History
history of large caffeine consumption or direct correlation between caffeine intake and palpitations
Exam
physical examination is nonspecific
1st investigation
- none:
diagnosis is based on clinical evaluation
More
Other investigations
QT prolonging drugs
History
use of stimulants or medications that prolong the QT interval such as fluoroquinolone antibiotics or certain antipsychotics
Exam
physical examination is nonspecific
1st investigation
- none:
diagnosis is based on clinical evaluation
Other investigations
- ECG:
to exclude acquired long QT syndrome
Postural orthostatic tachycardia syndrome (POTS)
History
usually young women age 15 to 25 years, may be recent viral infection; symptoms related to orthostatic intolerance (palpitations, lightheadedness, blurred vision, exercise intolerance, presyncope and syncope, tremor, generalized weakness, fatigue); may also present with nonorthostatic symptoms including dyspnea, gastrointestinal symptoms (e.g., bloating, nausea, diarrhea, constipation, abdominal pain), exercise intolerance, fatigue, headache, sleep disturbance, cognitive impairment, chest pain, bladder disturbance; may present with symptoms of associated comorbidities, such as Ehlers-Danlos syndrome and autoimmune diseases, particularly Hashimotos thyroiditis and celiac disease
Exam
orthostatic tachycardia, orthostatic palpitations; signs of associated comorbidities (e.g., joint hypermobility, small nontender goiter, diarrhea)
1st investigation
- 10 minute standing test:
heart rate increased by ≥30 bpm ( ≥40 bpm in patients ages 12 to 19 years old) after changing position from supine to standing, and no orthostatic hypotension (sustained drop in systolic blood pressure by ≥20 mmHg)
More - CBC:
normal
More - thyroid function tests:
normal
More - electrolytes:
normal
More
Other investigations
- 24-hour Holter monitor:
tachycardia induced by orthostatic changes; no supraventricular arrhythmias
- tilt-table test:
orthostatic tachycardia with changing position
More
Uncommon
Inappropriate sinus tachycardia
History
exaggerated heart response to exercise, without an identifiable etiology for the tachycardia such as pregnancy, anemia, or hyperthyroidism; commonly seen in young women
Exam
normal except for a fast and regular pulse >100 bpm
1st investigation
- ECG:
normal except for a resting rate of >100 bpm
Other investigations
- pregnancy test:
negative
- thyroid stimulating hormone:
normal
- CBC:
normal
Idiopathic ventricular tachycardia
History
paroxysmal palpitations; often seen in the setting of catecholamine excess such as vigorous exercise; can be associated with near-syncope; typically no family history of arrhythmia
Exam
typically normal except during palpitations when the patient may have salvos of nonsustained VT that manifest as a rapid regular pulse
1st investigation
- ECG (at baseline):
normal
Other investigations
- event monitor or ECG in arrhythmia:
wide complex tachycardia; when due to right ventricular outflow tract VT it has a left bundle branch block (LBBB)/inferior axis morphology, when due to left ventricular VT it has an LBBB or right bundle branch block (RBBB) with inferior axis; left ventricular VT has a relatively narrow RBBB typically with a superior axis
- echocardiogram:
normal
- serum electrolytes:
variable; electrolyte abnormalities (particularly hypokalemia and hypomagnesemia) often incite and/or contribute to VT; hypokalemia and hypomagnesemia frequently associated with torsades de pointes (polymorphic VT with a characteristic twisting morphology occurring in the setting of QT-interval prolongation)
Long QT syndrome
History
palpitations, often associated with syncope, can be triggered by exercise, fever, or emotional stress; drug history includes QT-prolonging drugs such as fluoroquinolone antibiotics or certain antipsychotics
Exam
typically normal
1st investigation
- baseline ECG without symptoms:
QT duration >450 ms in men and >470 ms in women with associated T-wave abnormalities
More

Other investigations
- ECG during tachycardia or event monitor:
nonsustained polymorphic VT
- echocardiogram:
normal
- serum electrolytes:
variable; electrolyte abnormalities (particularly hypokalemia and hypomagnesemia) often incite and/or contribute to VT; hypokalemia and hypomagnesemia frequently associated with torsades de pointes (polymorphic VT with a characteristic twisting morphology occurring in the setting of QT-interval prolongation)
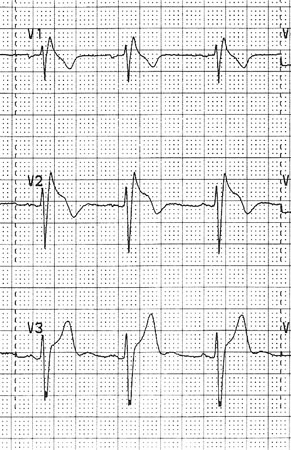
Brugada syndrome
History
patients can present between ages 22 and 65 years with palpitations due to episodes of nonsustained VT or ventricular fibrillation (VF); often associated with syncope
Exam
typically normal
1st investigation
- ECG:
type 1 Brugada pattern: coved ST-segment elevation (J-point elevation with a gradual down-sloping ST-segment) ≥2 mm with a negative T-wave in the right precordial leads. Type 2 or 3 Brugada pattern: saddleback ST-segment configuration with variable levels of ST-segment elevation
More - echocardiogram:
normal; mild structural abnormalities in the right ventricle or right ventricular outflow tract
Other investigations
- provocative drug testing with sodium channel blockade:
development of type 1 Brugada pattern on ECG: coved ST-segment elevation (J-point elevation with a gradual down-sloping ST-segment) ≥2 mm with a negative T-wave in the right precordial leads
More - genetic testing:
may be positive for known pathogenic mutation associated with Brugada syndrome (e.g., SCN5A)
More
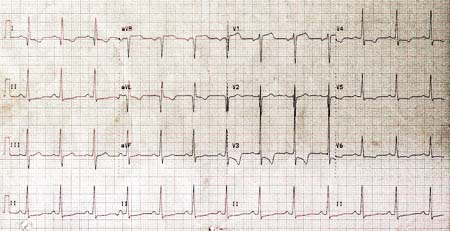
Hypertrophic cardiomyopathy
History
family history of hypertrophic cardiomyopathy or sudden cardiac death; symptoms are associated with dyspnea on exertion, near-syncope, and syncope, most often due to atrial fibrillation, but also VT
Exam
harsh crescendo-decrescendo murmur heard best in the right upper sternal border that gets louder with Valsalva maneuver, going from squatting to standing, or after a premature ventricular contraction; signs and symptoms of heart failure can be present, but typically not until later in the disease course
1st investigation
- baseline ECG without symptoms:
deep septal Q waves in I, VL, and V4 through V6; suggest marked left ventricular hypertrophy due to hypertrophic obstructive cardiomyopathy
More
Other investigations
- ECG (if tachycardic) or event monitor:
premature ventricular contractions; nonsustained VT; sustained VT (uncommon)
- echocardiogram:
left ventricular hypertrophy with intracavitary pressure gradient, systolic anterior motion of the anterior mitral valve leaflet
- serum electrolytes:
variable; electrolyte abnormalities (particularly hypokalemia and hypomagnesemia) often incite and/or contribute to VT; hypokalemia and hypomagnesemia frequently associated with torsades de pointes (polymorphic VT with a characteristic twisting morphology occurring in the setting of QT-interval prolongation)
VT in the setting of other structural heart disease
History
history of coronary heart disease with myocardial infarction, repaired congenital heart disease, mitral valve prolapse and/or regurgitation
Exam
signs of cardiomyopathy and/or congestive heart failure; diffuse and/or laterally displaced apical impulse consistent with left ventricular enlargement; gallop rhythm (S3); signs of atherosclerosis such as arterial bruits
1st investigation
- baseline ECG without symptoms:
old Q-wave infarction
Other investigations
- ECG (if tachycardic) or event monitor:
VT or ventricular ectopy with a QRS morphology consistent with a focus from a prior infarction, that is, QRS complexes with a right bundle/superior axis in a patient with a prior inferior wall infarction
- echocardiogram:
depressed left ventricular ejection fraction either with regional wall motion abnormalities suggestive of infarction or diffuse hypokinesis in the case of noncoronary cardiomyopathy
- serum electrolytes:
variable; electrolyte abnormalities (particularly hypokalemia and hypomagnesemia) often incite and/or contribute to VT; hypokalemia and hypomagnesemia frequently associated with torsades de pointes (polymorphic VT with a characteristic twisting morphology occurring in the setting of QT-interval prolongation)
Pheochromocytoma
History
headaches, flushing, diaphoresis, resistant hypertension, family history of panic attack-like symptoms (but episodic rather than situational)
Exam
hypertension, sinus tachycardia
1st investigation
- 24-hour urine collection for catecholamines, metanephrines, normetanephrines, and creatinine:
elevated
- serum-free metanephrines and normetanephrines:
elevated
- plasma catecholamines:
may be elevated
Other investigations
- ECG:
normal or tachyarrhythmia
Use of this content is subject to our disclaimer