History and exam
Key diagnostic factors
common
oral ulcers
Minor aphthae are found mainly on the nonkeratinized mucosa of the lips, cheeks, floor of the mouth, sulci, or ventrum of the tongue. They are less than 10 mm in diameter, occur in groups of 1 to 6 at a time, and tend to heal within 7-10 days without scarring.[1][2][6][Figure caption and citation for the preceding image starts]: Recurrent aphthous stomatitis (RAS): minor aphthaeFrom the personal collection of Crispian Scully, MD, PhD, FDSRCS, FRCPath [Citation ends].
Major aphthae involve any oral site, including the keratinized mucosa (palate and dorsum of tongue). They are round or ovoid ulcers greater than 10 mm in diameter, and occur in groups of 1 to 6 at a time. They are often more painful and persistent than minor aphthae and heal slowly, over 10-40 days, or occasionally longer.[1][2][6][Figure caption and citation for the preceding image starts]: Recurrent aphthous stomatitis (RAS): major aphthaeFrom the personal collection of Crispian Scully, MD, PhD, FDSRCS, FRCPath [Citation ends].
Herpetiform aphthous ulcers are rarer than major and minor aphthous ulcers and typically present as multiple (5-100) pinhead-sized discrete ulcers that can increase in size and coalesce to leave large areas of ulceration. They mimic herpes simplex stomatitis, but are not preceded by vesicles or blistering, and are not communicable. They are often extremely painful. They can involve any oral site, including the keratinized mucosa (palate and dorsum of tongue). They heal in 10 days or longer and recur so frequently that ulceration may seem continuous. They occur in a slightly older age group than the other forms of recurrent aphthous stomatitis and mainly in women.[1][2][6][Figure caption and citation for the preceding image starts]: Recurrent aphthous stomatitis (RAS): herpetiform ulcerationFrom: Scully C, Flint S, Porter SR, et al. Oral and Maxillofacial diseases. London UK; 2004. Used with permission [Citation ends].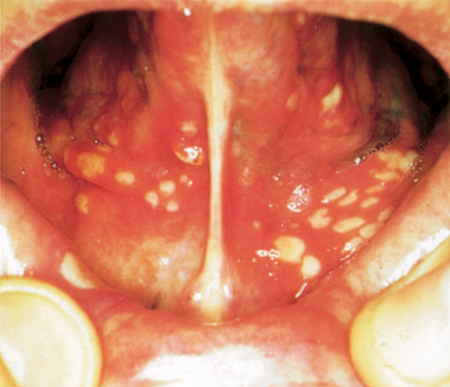
afebrile
Periodic/recurrent fevers suggest an alternate systemic condition (e.g., cyclic neutropenia, periodic fever with aphthae, pharyngitis, and adenitis [PFAPA syndrome], or tumor necrosis factor receptor-associated periodic syndrome).
absence of genital or ocular ulceration
no history of immunodeficiency
Immunodeficiency (including HIV infection) suggests aphthous-like ulceration rather than recurrent aphthous stomatitis.[6]
absence of pallor
Anemia leading to pallor, fatigue, weakness, decreased exercise tolerance, and shortness of breath with exercise may result from an underlying hematinic deficiency.
Pallor may also suggest iron deficiency anemia as a cause of aphthous-like ulceration if accompanied by glossitis, angular stomatitis, and spooning of the nails.
Risk factors
strong
positive family history
Over 42% of recurrent aphthous stomatitis (RAS) patients have first-degree relatives with RAS.[1][10]
The likelihood of childhood-onset RAS is 90% when both parents are affected but only 20% when neither parent has RAS.
RAS is more severe and starts at an earlier age in patients with a positive family history.[1]
nonsmoker or cessation of smoking
Patients with recurrent aphthous stomatitis are usually nonsmokers and there is a lower prevalence and severity of ulcers in heavy compared with moderate smokers.[15][16]
Some patients report an onset of ulcers parallel to smoking cessation, whereas others report control on reinitiation of smoking. The use of smokeless tobacco is also associated with a significantly lower prevalence of ulcers. Nicotine-containing tablets also appear to control the frequency of aphthae.[6]
weak
cows' milk-fed children
Recurrent aphthous stomatitis (RAS) may be more prevalent in cows' milk-fed children.[20] There is still no conclusive evidence to support environmental allergens or food hypersensitivities as a major cause of RAS.
high stress levels
food intolerance
Certain foods (e.g., chocolate, peanuts, coffee, and gluten products) have been reported to trigger episodes of recurrent aphthous stomatitis.[3]
hormonal imbalance
There are patients whose ulcers coincide with the luteal phase of the menstrual cycle and often remit with oral contraceptives or during pregnancy.[6]
use of sodium lauryl sulfate-containing toothpaste
An increased frequency of recurrent aphthous stomatitis (RAS) related to sodium lauryl sulfate (SLS)-containing dentifrice has been reported, although other studies found no such association.[21]
Because SLS dentifrices are in widespread use, it seems unlikely that this agent truly predisposes to, or causes, most RAS.[6]
Use of this content is subject to our disclaimer