Approach
Diagnosis is based on the history and clinical examination. There are no specific laboratory findings. It is important, however, to consider and exclude any possible systemic cause for recurrent ulcers, such as celiac disease, especially in people with systemic symptoms or signs, or adults with no prior history of oral ulceration.[1][6] Furthermore, a solitary ulcer lasting more than 3 weeks may well represent malignancy and would warrant urgent referral to a specialist.[29] This will require further investigation and may involve incisional biopsy.
History
The onset of recurrent aphthous stomatitis (RAS) is usually during childhood; in 80% of cases, it develops before 30 years of age. History should include detailing the episodic pattern/cyclic nature of ulceration, number of ulcers, duration, age of onset, and any associated trigger factors. A family history is of value as over 42% of patients have first-degree relatives with RAS.[1][10] RAS is more severe and starts at an earlier age in patients with a positive family history.[1] Trigger factors for onset of an episode of active ulceration may include trauma (e.g., following over-vigorous tooth brushing) and certain foods (e.g., chocolate, peanuts, coffee, and gluten products).[3] In some patients, ulcers coincide with the luteal phase of the menstrual cycle and often remit with oral contraceptives or during pregnancy.[6]
Clinical examination
Ulcers typically occur on the nonkeratinized oral mucosa: the buccal and labial mucosae, floor of the mouth, or ventrum of the tongue. There are three clinical presentations of RAS.[1][2][6]
Minor aphthous ulcers account for 75% to 85% of all RAS cases. These are less than 10 mm in diameter and tend to heal within 7-10 days without scarring. They are found mainly on the nonkeratinized mucosa of the lips, cheeks, floor of the mouth, sulci, or ventrum of the tongue.[Figure caption and citation for the preceding image starts]: Recurrent aphthous stomatitis (RAS): minor aphthaeFrom the personal collection of Crispian Scully, MD, PhD, FDSRCS, FRCPath [Citation ends].

Major aphthous ulcers (10% to 15% of all RAS cases) are round or ovoid and are greater than 10 mm in diameter. They are often more painful and persistent than minor aphthae. They involve any oral site, including the keratinized mucosa (palate and dorsum of tongue). They occur in groups of 1 to 6 at a time. They heal slowly over 10-40 days, or occasionally longer, recur frequently, and may heal with scarring.[Figure caption and citation for the preceding image starts]: Recurrent aphthous stomatitis (RAS): major aphthaeFrom the personal collection of Crispian Scully, MD, PhD, FDSRCS, FRCPath [Citation ends].

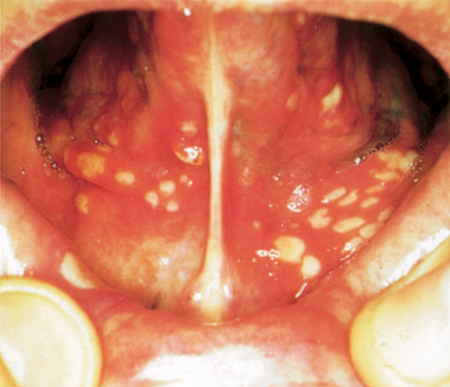
Herpetiform aphthous ulcers are rarer than major and minor aphthous ulcers and typically present as multiple (5-100) pinhead-sized discrete ulcers that can increase in size and coalesce to leave large areas of ulceration. They mimic herpes simplex stomatitis, but are not preceded by vesicles or blistering, and are not communicable. They are often extremely painful. They can involve any oral site, including the keratinized mucosa (palate and dorsum of tongue). They heal in 10 days or longer and recur so frequently that ulceration may seem continuous. They occur in a slightly older age group than the other forms of RAS and mainly in women.[Figure caption and citation for the preceding image starts]: Recurrent aphthous stomatitis (RAS): herpetiform ulcerationFrom: Scully C, Flint S, Porter SR, et al. Oral and Maxillofacial diseases. London UK; 2004. Used with permission [Citation ends].
Oral ulceration similar in clinical appearance to RAS (aphthous-like ulceration [ALU]) can present as a manifestation of a number of systemic disorders.
ALU may occur in immunodeficiency states including HIV infection or neutrophil dysfunction (e.g., as a component of cyclic neutropenia).[6][30]
ALU may occur in Behcet syndrome. These patients may present with, or have a history of, aphthous-like ulcers occurring on genital or other mucosae; erythema nodosum or other skin lesions; uveitis; joint involvement; or central nervous system manifestations.[1][31] In MAGIC (mouth and genital ulcers with inflamed cartilage) syndrome, a variant of Behcet syndrome, a generalized chondritis may be present along with major aphthae.[32]
Other autoinflammatory states in which ALU may present include periodic fever with aphthae, pharyngitis, and adenitis (PFAPA syndrome), and tumor necrosis factor receptor-associated periodic syndrome.[33][34] In these patients, fever is characteristic; cutaneous and other lesions may also be present, such as cervical lymphadenopathy.
Hematinic (iron, folic acid, or vitamin B12) deficiencies may also present with ALU as a component of the underlying anemia, or in pre-anemia, often with angular stomatitis and/or sore tongue. Pallor, fatigue, weakness, decreased exercise tolerance, and shortness of breath with exercise may result from anemia per se and should be ascertained from the history. Assessment of other signs of iron deficiency (e.g., glossitis, angular stomatitis, and spooning of the nails) should be made. In patients with B12 deficiency, a wide range of other signs and symptoms may be present. A history of diet poor in sources of folate and phenytoin or heavy alcohol use may suggest folate deficiency.
ALU can also be a feature of inflammatory bowel disease, both of Crohn disease and less commonly of ulcerative colitis and celiac disease. In these patients, the ulceration probably often reflects the associated hematinic deficiencies.[6][35]
A full medication history should be taken. ALU has been reported in patients taking nonsteroidal anti-inflammatory drugs, beta-blockers, nicorandil (a potassium channel blocker), ACE inhibitors, antibiotics, anticonvulsants, anticoagulants, and methotrexate.[1][36]
Laboratory investigations
Although there are no specific laboratory findings in RAS, in some patients - for example, where history and exam suggest a nutritional deficiency or a hematologic disorder - complete blood count and hematinic estimation (serum ferritin, serum/red cell folate, and serum B12) is indicated to exclude iron and vitamin deficiencies.[1] In patients of all age groups with suspected celiac disease, a serum immunoglobulin A-tissue transglutaminase may be an appropriate initial investigation. Testing for HIV infection should be considered in patients with a history of HIV-associated infections (candidiasis, hairy leukoplakia) or neoplasms (Kaposi sarcoma, lymphoma), or other clinical evidence of, or risk factors for, HIV infection.[1] An elevated plasma viscosity or erythrocyte sedimentation rate may be found in autoinflammatory states. In patients with abnormal results, a diagnosis of ALU is more likely than RAS. In these patients, definitive diagnosis will depend on subsequent investigations as appropriate. Symptoms of autoimmune disorder (e.g., skin lesions) alongside ulcers may warrant an antinuclear antibody test in order to rule out autoimmune disease.
A solitary ulcer lasting more than 3 weeks may well represent malignancy and would warrant urgent referral to a specialist.[29] This will require further investigation and may involve incisional biopsy.
Use of this content is subject to our disclaimer