Etiology
Passage of a hard stool bolus may precipitate an anal fissure. However, only a minority of patients are constipated at the onset of symptoms. The fissure may begin during an episode of loose stool or often occurs spontaneously with no obvious precipitating factor. Opiate analgesia is associated with constipation and a subsequent increased incidence of anal fissure.
The classical teaching is that the hard stool tears the anal skin from the pectin (at the dentate line), but alternative etiologic theories include ischemia in the anterior and posterior midline of the anal skin and a deficiency in the intrinsic nitric oxide synthase pathway.[6][7]
Pathophysiology
Anal fissure may be an ischemic ulcer.[6][8] Cadaveric studies of the blood supply to the anal canal show poor circulation in the posterior midline of the anal canal, where more than 90% of fissures occur.[9][10] This blood supply is further reduced by spasm of the internal anal sphincter. When a hard stool that tears the anal skin is passed, there is not sufficient blood supply to heal the split in the skin. Alternatively, the skin in the posterior midline breaks down with more minimal trauma and cannot heal.[11]
All treatments are aimed at reducing the spasm of the internal anal sphincter, which increases local blood flow and leads to the relief of symptoms and healing of the fissure. As spasm of the internal sphincter may be due to a local lack of nitric oxide synthase, application of organic nitrate ointment to the anus has been shown to effectively lower the anal resting pressure and improve pain on defecation, with healing occurring in 50% to 67%.[12][13] Similar results have been demonstrated for other agents reducing anal resting pressure such as calcium channel blockers and onabotulinumtoxinA (formerly known as botulinum toxin type A).[13] Surgery is a very effective means of reducing anal resting pressure by damage to the internal anal sphincter.
Classification
Timeframe
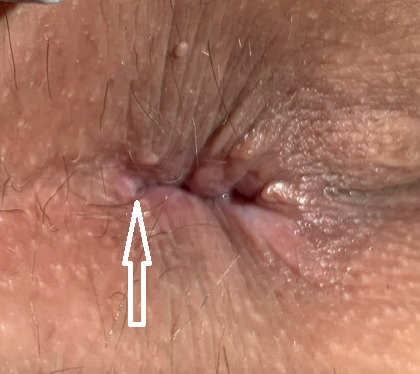
Acute: split in the skin of the distal anal canal.[2] The natural history suggests that many acute fissures spontaneously heal after 1 or 2 weeks, before medical attention is sought. A significant percentage do not, however, and over time persist and become chronic. [Figure caption and citation for the preceding image starts]: Acute anal fissureFrom the collection of Dr Nivedh Paluvoi, MD; used with permission [Citation ends].
Chronic: a fissure persisting for longer than 6 weeks, often showing other morphologic features such as indurated edges, a skin tag, and visible internal anal sphincter fibers at its base.[2]
[Figure caption and citation for the preceding image starts]: Chronic anal fissureFrom the collection of Dr Nivedh Paluvoi, MD; used with permission [Citation ends].

Use of this content is subject to our disclaimer