Pericarditis
- Overview
- Theory
- Diagnosis
- Management
- Follow up
- Resources
Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
Look out for this icon: for treatment options that are affected, or added, as a result of your patient's comorbidities.
suspected pericarditis
assess risk and consider admission to hospital
Any patient with a clinical presentation that suggests an underlying etiology should be admitted to hospital for further investigation and treatment.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Patients with at least one predictor of poor prognosis (major or minor risk factors below) should also be admitted.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com Patients with any of these risk factors warrant careful observation and follow-up.
Major risk factors include: high fever (i.e., >100.4°F [>38°C]); subacute course (i.e., symptoms over several days without a clear-cut acute onset); evidence of a large pericardial effusion (i.e., diastolic echo-free space >20 mm); cardiac tamponade; failure to respond within 7 days to a nonsteroidal anti-inflammatory drug (NSAID).
Minor risk factors include: pericarditis associated with myocarditis (myopericarditis); immunosuppression; trauma; oral anticoagulant therapy. Patients with any of these risk factors warrant careful observation and follow-up.
Some patients without any of these features can be managed as an outpatient if considered appropriate. In these cases, the patient should be started on treatment (i.e., empiric anti-inflammatories) with follow-up after 1 week to assess the response to treatment.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
pericardiocentesis
Treatment recommended for SOME patients in selected patient group
Pericardiocentesis is indicated for clinical tamponade, for high suspicion of purulent or neoplastic pericarditis, or for large or symptomatic effusions.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
purulent
pericardiocentesis + intravenous antibiotics
Purulent pericarditis is immediately life-threatening and requires immediate confirmation of diagnosis via urgent pericardiocentesis. Pericardial fluid should be tested for bacterial, fungal, and tuberculous causes, and blood should be drawn for culture.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Urgent rinsing of the pericardial cavity and intravenous antibiotics are mandatory.[37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Empiric intravenous antibiotic therapy is recommended until microbiologic results are available. There are limited data available to guide selection of the best empiric regimen, but experts typically recommend a regimen that contains an antistaphylococcal antibiotic. The choice of antibiotics will depend on various factors including local resistance patterns and MRSA prevalence. Follow your local protocols for choice of antibiotics and seek microbiology or infectious disease advice. Empiric therapy should be switched to tailored therapy depending on the underlying pathogens identified from pericardial fluid and blood cultures.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Therapy with systemic antibiotics should be continued until fever and clinical signs of infection, including leukocytosis, have resolved.
Plus – nonsteroidal anti-inflammatory drug (NSAID) or alternative analgesia![]()
nonsteroidal anti-inflammatory drug (NSAID) or alternative analgesia
Treatment recommended for ALL patients in selected patient group
An NSAID should be started immediately on diagnosis for symptom management.[16]Khandaker MH, Espinosa RE, Nishimura RA, et al. Pericardial disease: diagnosis and management. Mayo Clin Proc. 2010 Jun;85(6):572-93. http://www.ncbi.nlm.nih.gov/pubmed/20511488?tool=bestpractice.com [20]Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015 Oct 13;314(14):1498-506. https://iris.unito.it/handle/2318/1576078#.XAFHbdv7S70 http://www.ncbi.nlm.nih.gov/pubmed/26461998?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [57]Galluzzo A, Imazio M. Advances in medical therapy for pericardial diseases. Expert Rev Cardiovasc Ther. 2018 Sep;16(9):635-43. http://www.ncbi.nlm.nih.gov/pubmed/30103638?tool=bestpractice.com Consider tapering the dose after 1-2 weeks according to symptoms.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com NSAIDs reduce fever, chest pain, and inflammation but do not prevent tamponade, constriction, or recurrent pericarditis.[37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Choice of drug is based on patient characteristics (e.g., contraindications, previous efficacy, or side effects), the presence of concomitant diseases (e.g., aspirin is favored over other NSAIDs if antiplatelet therapy is required), and physician expertise.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Alternatively, acetaminophen or an opioid (e.g., codeine) can be considered if NSAIDs are not effective or are contraindicated.
Primary options
ibuprofen: 600 mg orally every 8 hours for 1-2 weeks, then decrease dose by 200-400 mg every 1-2 weeks
OR
aspirin: 750-1000 mg orally every 8 hours for 1-2 weeks, then decrease dose by 250-500 mg every 1-2 weeks
Secondary options
acetaminophen: 325-1000 mg orally every 4-6 hours when required, maximum 4000 mg/day
OR
codeine sulfate: 15-60 mg orally every 4-6 hours when required, maximum 360 mg/day
These drug options and doses relate to a patient with no comorbidities.
Primary options
ibuprofen: 600 mg orally every 8 hours for 1-2 weeks, then decrease dose by 200-400 mg every 1-2 weeks
OR
aspirin: 750-1000 mg orally every 8 hours for 1-2 weeks, then decrease dose by 250-500 mg every 1-2 weeks
Secondary options
acetaminophen: 325-1000 mg orally every 4-6 hours when required, maximum 4000 mg/day
OR
codeine sulfate: 15-60 mg orally every 4-6 hours when required, maximum 360 mg/day
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
ibuprofen
OR
aspirin
Secondary options
acetaminophen
OR
codeine sulfate
exercise restriction
Treatment recommended for ALL patients in selected patient group
Exercise should be restricted until chest pain resolves and inflammatory markers have normalized.[55]Kim JH, Baggish AL, Levine BD, et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2025 Feb 20 [Epub ahead of print]. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001297 http://www.ncbi.nlm.nih.gov/pubmed/39973614?tool=bestpractice.com A minimum of 3 months is often considered appropriate (and recommended for patients involved in competitive sports), but shorter periods of exercise restriction may be considered depending on patient and disease characteristics (e.g., nonathletes and/or mild clinical picture).[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [56]Pelliccia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2019 Jan 1;40(1):19-33. https://academic.oup.com/eurheartj/article/40/1/19/5248228 http://www.ncbi.nlm.nih.gov/pubmed/30561613?tool=bestpractice.com
proton-pump inhibitor
Treatment recommended for SOME patients in selected patient group
Due to the high doses of NSAIDs used, a proton-pump inhibitor (e.g., esomeprazole, lansoprazole) is given alongside NSAID therapy (if used) to protect against gastrointestinal ulcer formation.[12]Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004 Nov 18;351(21):2195-202. http://www.ncbi.nlm.nih.gov/pubmed/15548780?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Primary options
esomeprazole: 20-40 mg orally once daily
OR
lansoprazole: 15-30 mg orally once daily
These drug options and doses relate to a patient with no comorbidities.
Primary options
esomeprazole: 20-40 mg orally once daily
OR
lansoprazole: 15-30 mg orally once daily
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
esomeprazole
OR
lansoprazole
colchicine
Treatment recommended for SOME patients in selected patient group
Should be used with caution in patients with purulent pericarditis as it may interfere with leukocyte function and infection clearance.[54]McEwan T, Robinson PC. A systematic review of the infectious complications of colchicine and the use of colchicine to treat infections. Semin Arthritis Rheum. 2021 Feb;51(1):101-12. https://www.doi.org/10.1016/j.semarthrit.2020.11.007 http://www.ncbi.nlm.nih.gov/pubmed/33360321?tool=bestpractice.com
It is given for 3 months in the setting of acute pericarditis.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [20]Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015 Oct 13;314(14):1498-506. https://iris.unito.it/handle/2318/1576078#.XAFHbdv7S70 http://www.ncbi.nlm.nih.gov/pubmed/26461998?tool=bestpractice.com [57]Galluzzo A, Imazio M. Advances in medical therapy for pericardial diseases. Expert Rev Cardiovasc Ther. 2018 Sep;16(9):635-43. http://www.ncbi.nlm.nih.gov/pubmed/30103638?tool=bestpractice.com [60]Bayes-Genis A, Adler Y, de Luna AB, et al. Colchicine in pericarditis. Eur Heart J. 2017 Jun 7;38(22):1706-9. https://www.doi.org/10.1093/eurheartj/ehx246 http://www.ncbi.nlm.nih.gov/pubmed/30052886?tool=bestpractice.com
While tapering the dose is not mandatory, it can be considered in the last few weeks of treatment to prevent persistence of symptoms and recurrence.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Before commencing treatment, a baseline complete blood count (CBC) is indicated as colchicine may cause neutropenia and bone marrow suppression. Caution should be exercised in renal and hepatic impairment as its use may be contraindicated in patients on certain medications.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
These drug options and doses relate to a patient with no comorbidities.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
colchicine
pericardiotomy/pericardiectomy
Open surgical drainage via a subxiphoid pericardiotomy should be considered.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Pericardiectomy is necessary in the presence of dense adhesions or loculations, persistent bacteremia, recurrent tamponade, or progression to constrictive physiology.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64.
http://eurheartj.oxfordjournals.org/content/36/42/2921.long
http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
[37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28.
http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: Open surgery in a baby with purulent pericarditis; the abscess is indicated by the arrowKaruppaswamy V, Shauq A, Alphonso N. BMJ Case Reports 2009; doi:10.1136/bcr.2007.136564 [Citation ends].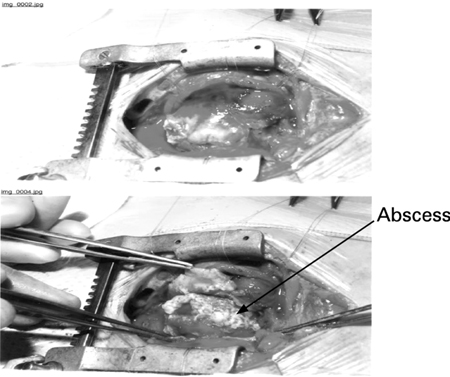
non-purulent
1st line – nonsteroidal anti-inflammatory drug (NSAID) or alternative analgesia![]()
nonsteroidal anti-inflammatory drug (NSAID) or alternative analgesia
An NSAID should be started immediately on diagnosis for symptom management.[16]Khandaker MH, Espinosa RE, Nishimura RA, et al. Pericardial disease: diagnosis and management. Mayo Clin Proc. 2010 Jun;85(6):572-93. http://www.ncbi.nlm.nih.gov/pubmed/20511488?tool=bestpractice.com [20]Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015 Oct 13;314(14):1498-506. https://iris.unito.it/handle/2318/1576078#.XAFHbdv7S70 http://www.ncbi.nlm.nih.gov/pubmed/26461998?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [57]Galluzzo A, Imazio M. Advances in medical therapy for pericardial diseases. Expert Rev Cardiovasc Ther. 2018 Sep;16(9):635-43. http://www.ncbi.nlm.nih.gov/pubmed/30103638?tool=bestpractice.com Consider tapering the dose after 1-2 weeks according to symptoms.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com NSAIDs reduce fever, chest pain, and inflammation but do not prevent tamponade, constriction, or recurrent pericarditis.[37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Choice of drug is based on patient characteristics (e.g., contraindications, previous efficacy, or side effects), the presence of concomitant diseases (e.g., aspirin is favored over other NSAIDs if antiplatelet therapy is required), and physician expertise.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Alternatively, acetaminophen or an opioid (e.g., codeine) can be considered if NSAIDs are not effective or are contraindicated.
Primary options
ibuprofen: 600 mg orally every 8 hours for 1-2 weeks, then decrease dose by 200-400 mg every 1-2 weeks
OR
aspirin: 750-1000 mg orally every 8 hours for 1-2 weeks, then decrease dose by 250-500 mg every 1-2 weeks
Secondary options
acetaminophen: 325-1000 mg orally every 4-6 hours when required, maximum 4000 mg/day
OR
codeine sulfate: 15-60 mg orally every 4-6 hours when required, maximum 360 mg/day
These drug options and doses relate to a patient with no comorbidities.
Primary options
ibuprofen: 600 mg orally every 8 hours for 1-2 weeks, then decrease dose by 200-400 mg every 1-2 weeks
OR
aspirin: 750-1000 mg orally every 8 hours for 1-2 weeks, then decrease dose by 250-500 mg every 1-2 weeks
Secondary options
acetaminophen: 325-1000 mg orally every 4-6 hours when required, maximum 4000 mg/day
OR
codeine sulfate: 15-60 mg orally every 4-6 hours when required, maximum 360 mg/day
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
ibuprofen
OR
aspirin
Secondary options
acetaminophen
OR
codeine sulfate
colchicine
Treatment recommended for ALL patients in selected patient group
Improves response, decreases recurrence, and increases remission rates.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [59]Andreis A, Imazio M, Casula M, et al. Colchicine efficacy and safety for the treatment of cardiovascular diseases. Intern Emerg Med. 2021 Sep;16(6):1691-700. https://link.springer.com/article/10.1007/s11739-021-02654-7 http://www.ncbi.nlm.nih.gov/pubmed/33704674?tool=bestpractice.com It is given for 3 months in this setting.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [20]Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015 Oct 13;314(14):1498-506. https://iris.unito.it/handle/2318/1576078#.XAFHbdv7S70 http://www.ncbi.nlm.nih.gov/pubmed/26461998?tool=bestpractice.com [57]Galluzzo A, Imazio M. Advances in medical therapy for pericardial diseases. Expert Rev Cardiovasc Ther. 2018 Sep;16(9):635-43. http://www.ncbi.nlm.nih.gov/pubmed/30103638?tool=bestpractice.com [60]Bayes-Genis A, Adler Y, de Luna AB, et al. Colchicine in pericarditis. Eur Heart J. 2017 Jun 7;38(22):1706-9. https://www.doi.org/10.1093/eurheartj/ehx246 http://www.ncbi.nlm.nih.gov/pubmed/30052886?tool=bestpractice.com
While tapering the dose is not mandatory, it can be considered in the last few weeks of treatment to prevent persistence of symptoms and recurrence.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Before commencing treatment, a baseline complete blood count (CBC) is indicated as colchicine may cause neutropenia and bone marrow suppression. Caution should be exercised in renal and hepatic impairment as its use may be contraindicated in patients on certain medications.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
These drug options and doses relate to a patient with no comorbidities.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
colchicine
exercise restriction
Treatment recommended for ALL patients in selected patient group
Exercise should be restricted until chest pain resolves and inflammatory markers have normalized.[55]Kim JH, Baggish AL, Levine BD, et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2025 Feb 20 [Epub ahead of print]. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001297 http://www.ncbi.nlm.nih.gov/pubmed/39973614?tool=bestpractice.com A minimum of 3 months is often considered appropriate (and recommended for patients involved in competitive sports), but shorter periods of exercise restriction may be considered depending on patient and disease characteristics (e.g., nonathletes and/or mild clinical picture).[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [56]Pelliccia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2019 Jan 1;40(1):19-33. https://academic.oup.com/eurheartj/article/40/1/19/5248228 http://www.ncbi.nlm.nih.gov/pubmed/30561613?tool=bestpractice.com
proton-pump inhibitor
Treatment recommended for SOME patients in selected patient group
Due to the high doses of NSAIDs used, a proton-pump inhibitor (e.g., esomeprazole, lansoprazole) is given alongside NSAID therapy (if used) to protect against gastrointestinal ulcer formation.[12]Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004 Nov 18;351(21):2195-202. http://www.ncbi.nlm.nih.gov/pubmed/15548780?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Primary options
esomeprazole: 20-40 mg orally once daily
OR
lansoprazole: 15-30 mg orally once daily
These drug options and doses relate to a patient with no comorbidities.
Primary options
esomeprazole: 20-40 mg orally once daily
OR
lansoprazole: 15-30 mg orally once daily
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
esomeprazole
OR
lansoprazole
corticosteroid
A corticosteroid can be considered in patients who do not respond to anti-inflammatory therapy or in whom an NSAID is contraindicated, once an infectious cause has been excluded. Corticosteroids are not recommended in patients with viral pericarditis because of the risk of re-activation of viral infection and ongoing inflammation. Corticosteroids may also be used when there is a specific indication for their use (e.g., presence of an autoimmune disease).[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
They are used in combination with colchicine for this indication.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Corticosteroids are less favored compared to NSAIDs because of the risks of promoting chronic and/or recurrent disease, and side effects.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
If used, low to moderate doses are preferred over high doses.[18]Chiabrando JG, Bonaventura A, Vecchié A, et al. Management of acute and recurrent pericarditis: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020 Jan 7;75(1):76-92. https://www.sciencedirect.com/science/article/pii/S0735109719384840?via%3Dihub http://www.ncbi.nlm.nih.gov/pubmed/31918837?tool=bestpractice.com The initial dose should be maintained until symptoms have resolved and the C-reactive protein (CRP) level has normalized. Once this is achieved, the dose may be gradually tapered.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Primary options
prednisone: 0.25 to 0.5 mg/kg/day orally, taper gradually after resolution of symptoms and normalization of CRP
More prednisoneTapering regimen depends on the starting dose. Starting dose >50 mg/day (taper dose by 10 mg/day every 1-2 weeks); starting dose 25-50 mg/day (taper dose by 5-10 mg/day every 1-2 weeks); starting dose 15-25 mg/day (taper dose by 2.5 mg/day every 2-4 weeks); starting dose <15 mg/day (taper dose by 1.25 to 2.5 mg/day every 2-6 weeks).
These drug options and doses relate to a patient with no comorbidities.
Primary options
prednisone: 0.25 to 0.5 mg/kg/day orally, taper gradually after resolution of symptoms and normalization of CRP
More prednisoneTapering regimen depends on the starting dose. Starting dose >50 mg/day (taper dose by 10 mg/day every 1-2 weeks); starting dose 25-50 mg/day (taper dose by 5-10 mg/day every 1-2 weeks); starting dose 15-25 mg/day (taper dose by 2.5 mg/day every 2-4 weeks); starting dose <15 mg/day (taper dose by 1.25 to 2.5 mg/day every 2-6 weeks).
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
prednisone
colchicine
Treatment recommended for ALL patients in selected patient group
Improves response, decreases recurrence, and increases remission rates.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [59]Andreis A, Imazio M, Casula M, et al. Colchicine efficacy and safety for the treatment of cardiovascular diseases. Intern Emerg Med. 2021 Sep;16(6):1691-700. https://link.springer.com/article/10.1007/s11739-021-02654-7 http://www.ncbi.nlm.nih.gov/pubmed/33704674?tool=bestpractice.com It is given for 3 months in this setting.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [20]Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015 Oct 13;314(14):1498-506. https://iris.unito.it/handle/2318/1576078#.XAFHbdv7S70 http://www.ncbi.nlm.nih.gov/pubmed/26461998?tool=bestpractice.com [57]Galluzzo A, Imazio M. Advances in medical therapy for pericardial diseases. Expert Rev Cardiovasc Ther. 2018 Sep;16(9):635-43. http://www.ncbi.nlm.nih.gov/pubmed/30103638?tool=bestpractice.com [60]Bayes-Genis A, Adler Y, de Luna AB, et al. Colchicine in pericarditis. Eur Heart J. 2017 Jun 7;38(22):1706-9. https://www.doi.org/10.1093/eurheartj/ehx246 http://www.ncbi.nlm.nih.gov/pubmed/30052886?tool=bestpractice.com
While tapering the dose is not mandatory, it can be considered in the last few weeks of treatment to prevent persistence of symptoms and recurrence.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Before commencing treatment, a baseline complete blood count (CBC) is indicated as colchicine may cause neutropenia and bone marrow suppression. Caution should be exercised in renal and hepatic impairment as its use may be contraindicated in patients on certain medications.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
These drug options and doses relate to a patient with no comorbidities.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
colchicine
exercise restriction
Treatment recommended for ALL patients in selected patient group
Exercise should be restricted until chest pain resolves and inflammatory markers have normalized.[55]Kim JH, Baggish AL, Levine BD, et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2025 Feb 20 [Epub ahead of print]. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001297 http://www.ncbi.nlm.nih.gov/pubmed/39973614?tool=bestpractice.com A minimum of 3 months is often considered appropriate (and recommended for patients involved in competitive sports), but shorter periods of exercise restriction may be considered depending on patient and disease characteristics (e.g., nonathletes and/or mild clinical picture).[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [56]Pelliccia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2019 Jan 1;40(1):19-33. https://academic.oup.com/eurheartj/article/40/1/19/5248228 http://www.ncbi.nlm.nih.gov/pubmed/30561613?tool=bestpractice.com
treatment of the underlying cause
Underlying causes include viral infections (e.g., Coxsackie virus A9, B1-4, Echo 8, mumps, Epstein-Barr virus, cytomegalovirus, varicella, rubella, HIV, Parvo-19, SARS-CoV-2), tuberculosis (a common cause in the developing world), secondary immune processes (e.g., rheumatic fever, postcardiotomy syndrome, post-myocardial infaction [MI] syndrome) metabolic disorders (e.g., uremia, myxedema), radiation therapy, cardiac surgery, percutaneous cardiac interventions, systemic autoimmune disorders (e.g., rheumatoid arthritis, systemic sclerosis, reactive arthritis, familial Mediterranean fever, systemic vasculitides, inflammatory bowel disease), bacterial/fungal/parasitic infections, trauma, certain drugs, and neoplasms. Patients with viral pericarditis may benefit from specific antiviral therapy; however, an infectious disease attending should be involved.
In patients with tuberculous pericarditis, first-line treatment is 4 to 6 weeks of antituberculous therapy.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64.
http://eurheartj.oxfordjournals.org/content/36/42/2921.long
http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
When tuberculous pericarditis is confirmed in a nonendemic area, a suitable 6-month regimen is effective; empiric therapy is not required in the absence of an established diagnosis in nonendemic areas.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64.
http://eurheartj.oxfordjournals.org/content/36/42/2921.long
http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Adjunctive therapies such as colchicine, corticosteroids, and immunotherapy have not been shown to be beneficial.[62]Mayosi BM, Ntsekhe M, Bosch J, et al. Prednisolone and Mycobacterium indicus pranii in tuberculous pericarditis. N Engl J Med. 2014 Sep 18;371(12):1121-30.
http://www.nejm.org/doi/full/10.1056/NEJMoa1407380#t=article
http://www.ncbi.nlm.nih.gov/pubmed/25178809?tool=bestpractice.com
[63]George IA, Thomas B, Sadhu JS. Systematic review and meta-analysis of adjunctive corticosteroids in the treatment of tuberculous pericarditis. Int J Tuberc Lung Dis. 2018 May 1;22(5):551-6.
http://www.ncbi.nlm.nih.gov/pubmed/29663961?tool=bestpractice.com
[64]Isiguzo G, Du Bruyn E, Howlett P, et al. Diagnosis and management of tuberculous pericarditis: what is new? Curr Cardiol Rep. 2020 Jan 15;22(1):2.
https://www.doi.org/10.1007/s11886-020-1254-1
http://www.ncbi.nlm.nih.gov/pubmed/31940097?tool=bestpractice.com
[65]Liebenberg JJ, Dold CJ, Olivier LR. A prospective investigation into the effect of colchicine on tuberculous pericarditis. Cardiovasc J Afr. 2016 Nov/Dec;27(6):350-5.
https://www.doi.org/10.5830/CVJA-2016-035
http://www.ncbi.nlm.nih.gov/pubmed/27965998?tool=bestpractice.com
However, corticosteroids may be considered in patients with tuberculous pericarditis who are HIV-negative.[66]Wiysonge CS, Ntsekhe M, Thabane L, et al. Interventions for treating tuberculous pericarditis. Cochrane Database Syst Rev. 2017 Sep 13;9:CD000526.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000526.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/28902412?tool=bestpractice.com
[ ![]() ]
What are the benefits and harms of steroids for people with tuberculous pericarditis?/cca.html?targetUrl=https://cochranelibrary.com/cca/doi/10.1002/cca.1937/fullShow me the answer Pericardiectomy is recommended if the patient does not improve or is deteriorating after 4 to 8 weeks of antituberculosis therapy.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64.
http://eurheartj.oxfordjournals.org/content/36/42/2921.long
http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
[67]Yadav S, Shah S, Iqbal Z, et al. Pericardiectomy for constrictive tuberculous pericarditis: a systematic review and meta-analysis on the etiology, patients' characteristics, and the outcomes. Cureus. 2021 Sep;13(9):e18252.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8544905
http://www.ncbi.nlm.nih.gov/pubmed/34722042?tool=bestpractice.com
]
What are the benefits and harms of steroids for people with tuberculous pericarditis?/cca.html?targetUrl=https://cochranelibrary.com/cca/doi/10.1002/cca.1937/fullShow me the answer Pericardiectomy is recommended if the patient does not improve or is deteriorating after 4 to 8 weeks of antituberculosis therapy.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64.
http://eurheartj.oxfordjournals.org/content/36/42/2921.long
http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
[67]Yadav S, Shah S, Iqbal Z, et al. Pericardiectomy for constrictive tuberculous pericarditis: a systematic review and meta-analysis on the etiology, patients' characteristics, and the outcomes. Cureus. 2021 Sep;13(9):e18252.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8544905
http://www.ncbi.nlm.nih.gov/pubmed/34722042?tool=bestpractice.com
Most patients with uremic pericarditis respond to intensive dialysis within 1 to 2 weeks.
Autoimmune disorders are treated with corticosteroids and/or another immunosuppressive therapy depending on the specific condition. Aspirin is preferred if required for persistent symptoms due to early pericarditis or late pericarditis post-MI as other NSAIDs adversely affect myocardial healing, and for its antiplatelet activity. Glucocorticoids and NSAIDs (other than aspirin) are not indicated for post-MI pericarditis due to the potential for harm.[58]Rao SV, O'Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI guideline for the management of patients with acute coronary syndromes: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. Mar 2025 [internet publication]. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001309 http://www.ncbi.nlm.nih.gov/pubmed/40014670?tool=bestpractice.com
Treatment of neoplasms may involve any combination of radiation therapy, chemotherapy, or surgery depending on the type of tumor identified.[37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Plus – nonsteroidal anti-inflammatory drug (NSAID) or alternative analgesia![]()
nonsteroidal anti-inflammatory drug (NSAID) or alternative analgesia
Treatment recommended for ALL patients in selected patient group
An NSAID should be started immediately on diagnosis for symptom management.[16]Khandaker MH, Espinosa RE, Nishimura RA, et al. Pericardial disease: diagnosis and management. Mayo Clin Proc. 2010 Jun;85(6):572-93. http://www.ncbi.nlm.nih.gov/pubmed/20511488?tool=bestpractice.com [20]Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015 Oct 13;314(14):1498-506. https://iris.unito.it/handle/2318/1576078#.XAFHbdv7S70 http://www.ncbi.nlm.nih.gov/pubmed/26461998?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [57]Galluzzo A, Imazio M. Advances in medical therapy for pericardial diseases. Expert Rev Cardiovasc Ther. 2018 Sep;16(9):635-43. http://www.ncbi.nlm.nih.gov/pubmed/30103638?tool=bestpractice.com Consider tapering the dose after 1-2 weeks according to symptoms.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com NSAIDs reduce fever, chest pain, and inflammation but do not prevent tamponade, constriction, or recurrent pericarditis.
Aspirin is the preferred NSAID in patients developing pericarditis after a myocardial infaction.[37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Alternatively, acetaminophen or an opioid (e.g., codeine) can be considered if NSAIDs are not effective or are contraindicated.
Primary options
ibuprofen: 600 mg orally every 8 hours for 1-2 weeks, then decrease dose by 200-400 mg every 1-2 weeks
OR
aspirin: 750-1000 mg orally every 8 hours for 1-2 weeks, then decrease dose by 250-500 mg every 1-2 weeks
Secondary options
acetaminophen: 325-1000 mg orally every 4-6 hours when required, maximum 4000 mg/day
OR
codeine sulfate: 15-60 mg orally every 4-6 hours when required, maximum 360 mg/day
These drug options and doses relate to a patient with no comorbidities.
Primary options
ibuprofen: 600 mg orally every 8 hours for 1-2 weeks, then decrease dose by 200-400 mg every 1-2 weeks
OR
aspirin: 750-1000 mg orally every 8 hours for 1-2 weeks, then decrease dose by 250-500 mg every 1-2 weeks
Secondary options
acetaminophen: 325-1000 mg orally every 4-6 hours when required, maximum 4000 mg/day
OR
codeine sulfate: 15-60 mg orally every 4-6 hours when required, maximum 360 mg/day
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
ibuprofen
OR
aspirin
Secondary options
acetaminophen
OR
codeine sulfate
exercise restriction
Treatment recommended for ALL patients in selected patient group
Exercise should be restricted until chest pain resolves and inflammatory markers have normalized.[55]Kim JH, Baggish AL, Levine BD, et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2025 Feb 20 [Epub ahead of print]. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001297 http://www.ncbi.nlm.nih.gov/pubmed/39973614?tool=bestpractice.com A minimum of 3 months is often considered appropriate (and recommended for patients involved in competitive sports), but shorter periods of restriction may be considered depending on patient and disease characteristics (e.g., nonathletes and/or mild clinical picture).[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [56]Pelliccia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2019 Jan 1;40(1):19-33. https://academic.oup.com/eurheartj/article/40/1/19/5248228 http://www.ncbi.nlm.nih.gov/pubmed/30561613?tool=bestpractice.com
colchicine
Treatment recommended for SOME patients in selected patient group
Improves response, decreases recurrence, and increases remission rates.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [59]Andreis A, Imazio M, Casula M, et al. Colchicine efficacy and safety for the treatment of cardiovascular diseases. Intern Emerg Med. 2021 Sep;16(6):1691-700. https://link.springer.com/article/10.1007/s11739-021-02654-7 http://www.ncbi.nlm.nih.gov/pubmed/33704674?tool=bestpractice.com It is given for 3 months in this setting.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [20]Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015 Oct 13;314(14):1498-506. https://iris.unito.it/handle/2318/1576078#.XAFHbdv7S70 http://www.ncbi.nlm.nih.gov/pubmed/26461998?tool=bestpractice.com [57]Galluzzo A, Imazio M. Advances in medical therapy for pericardial diseases. Expert Rev Cardiovasc Ther. 2018 Sep;16(9):635-43. http://www.ncbi.nlm.nih.gov/pubmed/30103638?tool=bestpractice.com [60]Bayes-Genis A, Adler Y, de Luna AB, et al. Colchicine in pericarditis. Eur Heart J. 2017 Jun 7;38(22):1706-9. https://www.doi.org/10.1093/eurheartj/ehx246 http://www.ncbi.nlm.nih.gov/pubmed/30052886?tool=bestpractice.com Not shown to be beneficial in patients with tuberculous pericarditis.[64]Isiguzo G, Du Bruyn E, Howlett P, et al. Diagnosis and management of tuberculous pericarditis: what is new? Curr Cardiol Rep. 2020 Jan 15;22(1):2. https://www.doi.org/10.1007/s11886-020-1254-1 http://www.ncbi.nlm.nih.gov/pubmed/31940097?tool=bestpractice.com [65]Liebenberg JJ, Dold CJ, Olivier LR. A prospective investigation into the effect of colchicine on tuberculous pericarditis. Cardiovasc J Afr. 2016 Nov/Dec;27(6):350-5. https://www.doi.org/10.5830/CVJA-2016-035 http://www.ncbi.nlm.nih.gov/pubmed/27965998?tool=bestpractice.com
Addition of colchicine should be considered in patients with postcardiotomy injury syndromes (e.g., Dressler syndrome, which generally occurs 1-2 weeks after a myocardial infaction [MI]; or postcardiac surgery), provided there are no contraindications and it is well tolerated. Preventive administration is recommended for 1 month. Careful follow-up with echocardiography every 6 to 12 months according to clinical features and symptoms should be considered to exclude possible evolution towards constrictive pericarditis.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
While tapering the dose is not mandatory, it can be considered in the last few weeks of treatment to prevent persistence of symptoms and recurrence.
Before commencing treatment, a baseline complete blood count (CBC) is indicated as colchicine may cause neutropenia and bone marrow suppression. Caution should be exercised in renal and hepatic impairment as its use may be contraindicated in patients on certain medications.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
These drug options and doses relate to a patient with no comorbidities.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
colchicine
proton-pump inhibitor
Treatment recommended for SOME patients in selected patient group
Due to the high doses of NSAIDs used, a proton-pump inhibitor (e.g., esomeprazole, lansoprazole) is given alongside NSAID therapy (if used) to protect against gastrointestinal ulcer formation.[12]Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004 Nov 18;351(21):2195-202. http://www.ncbi.nlm.nih.gov/pubmed/15548780?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Primary options
esomeprazole: 20-40 mg orally once daily
OR
lansoprazole: 15-30 mg orally once daily
These drug options and doses relate to a patient with no comorbidities.
Primary options
esomeprazole: 20-40 mg orally once daily
OR
lansoprazole: 15-30 mg orally once daily
Drug choice, dose and interactions may be affected by the patient's comorbidities. Check your local drug formulary.
Show drug information for a patient with no comorbidities
Primary options
esomeprazole
OR
lansoprazole
recurrent disease
1st line – nonsteroidal anti-inflammatory drug (NSAID) or alternative analgesia![]()
nonsteroidal anti-inflammatory drug (NSAID) or alternative analgesia
An NSAID should be started immediately on diagnosis for symptom management. NSAIDs reduce fever, chest pain, and inflammation but do not prevent tamponade, constriction, or recurrent pericarditis.[37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Choice of drug is based on patient characteristics (e.g., contraindications, previous efficacy, or side effects), the presence of concomitant diseases (e.g., aspirin is favored over other NSAIDs if antiplatelet therapy is required), and physician expertise. Aspirin is the preferred NSAID in patients developing pericarditis after a myocardial infarction (MI).[37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Alternatively, acetaminophen or an opioid (e.g., codeine) can be considered if NSAIDs are not effective or are contraindicated.
Treatment should be continued until symptoms resolve.
Primary options
ibuprofen: 600 mg orally every 8 hours for 1-2 weeks, then decrease dose by 200-400 mg every 1-2 weeks
OR
aspirin: 750-1000 mg orally every 8 hours for 1-2 weeks, then decrease dose by 250-500 mg every 1-2 weeks
Secondary options
acetaminophen: 325-1000 mg orally every 4-6 hours when required, maximum 4000 mg/day
OR
codeine sulfate: 15-60 mg orally every 4-6 hours when required, maximum 360 mg/day
colchicine
Treatment recommended for ALL patients in selected patient group
Improves response, decreases recurrence, and increases remission rates.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [59]Andreis A, Imazio M, Casula M, et al. Colchicine efficacy and safety for the treatment of cardiovascular diseases. Intern Emerg Med. 2021 Sep;16(6):1691-700. https://link.springer.com/article/10.1007/s11739-021-02654-7 http://www.ncbi.nlm.nih.gov/pubmed/33704674?tool=bestpractice.com
Treatment should be continued for 6 months in patients with recurrent disease. A longer duration of therapy can be considered in resistant cases. C-reactive protein (CRP) levels should be used to guide therapy and response. Once the CRP has normalized, drug therapy can be tapered gradually according to symptoms and the CRP level.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
While tapering the dose is not mandatory, it can be considered in the last few weeks of treatment to prevent persistence of symptoms and recurrence.
Before commencing treatment, a baseline complete blood count (CBC) is indicated as colchicine may cause neutropenia and bone marrow suppression. Caution should be exercised in renal and hepatic impairment as its use may be contraindicated in patients on certain medications.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
exercise restriction
Treatment recommended for ALL patients in selected patient group
Exercise should be restricted until chest pain resolves and inflammatory markers have normalized.[55]Kim JH, Baggish AL, Levine BD, et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2025 Feb 20 [Epub ahead of print]. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001297 http://www.ncbi.nlm.nih.gov/pubmed/39973614?tool=bestpractice.com A minimum of 3 months is often considered appropriate (and recommended for patients involved in competitive sports), but shorter periods of exercise restriction may be considered depending on patient and disease characteristics (e.g., nonathletes and/or mild clinical picture).[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [56]Pelliccia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2019 Jan 1;40(1):19-33. https://academic.oup.com/eurheartj/article/40/1/19/5248228 http://www.ncbi.nlm.nih.gov/pubmed/30561613?tool=bestpractice.com
treatment of the underlying cause
Treatment recommended for ALL patients in selected patient group
In addition, treatment should be directed at any known underlying cause.[37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
proton-pump inhibitor
Treatment recommended for SOME patients in selected patient group
Due to the high doses of NSAIDs used, a proton-pump inhibitor (e.g., esomeprazole, lansoprazole) is given alongside NSAID therapy (if used) to protect against gastrointestinal ulcer formation.[12]Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004 Nov 18;351(21):2195-202. http://www.ncbi.nlm.nih.gov/pubmed/15548780?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [38]Imazio M, Brucato A, Trinchero R, et al. Diagnosis and management of pericardial diseases. Nat Rev Cardiol. 2009 Dec;6(12):743-51. http://www.ncbi.nlm.nih.gov/pubmed/19859068?tool=bestpractice.com
Primary options
esomeprazole: 20-40 mg orally once daily
OR
lansoprazole: 15-30 mg orally once daily
corticosteroid
For patients who do not respond to an NSAID plus colchicine, corticosteroid therapy can be considered, once an infectious cause has been excluded. May also be used when there is a specific indication for their use (e.g., presence of an autoimmune disease). Should be used in combination with colchicine for this indication.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Less favored compared to NSAIDs because of the risks of promoting chronic and/or recurrent disease, and side effects.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
If used, low to moderate doses are preferred over high doses.[18]Chiabrando JG, Bonaventura A, Vecchié A, et al. Management of acute and recurrent pericarditis: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020 Jan 7;75(1):76-92. https://www.sciencedirect.com/science/article/pii/S0735109719384840?via%3Dihub http://www.ncbi.nlm.nih.gov/pubmed/31918837?tool=bestpractice.com The initial dose should be maintained until symptoms have resolved and the C-reactive protein (CRP) level has normalized. Once this is achieved, the dose may be gradually tapered.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
Primary options
prednisone: 0.25 to 0.5 mg/kg/day orally, taper gradually after resolution of symptoms and normalization of CRP
More prednisoneTapering regimen depends on the starting dose. Starting dose >50 mg/day (taper dose by 10 mg/day every 1-2 weeks); starting dose 25-50 mg/day (taper dose by 5-10 mg/day every 1-2 weeks); starting dose 15-25 mg/day (taper dose by 2.5 mg/day every 2-4 weeks); starting dose <15 mg/day (taper dose by 1.25 to 2.5 mg/day every 2-6 weeks).
colchicine
Treatment recommended for ALL patients in selected patient group
Improves response, decreases recurrence, and increases remission rates.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [59]Andreis A, Imazio M, Casula M, et al. Colchicine efficacy and safety for the treatment of cardiovascular diseases. Intern Emerg Med. 2021 Sep;16(6):1691-700. https://link.springer.com/article/10.1007/s11739-021-02654-7 http://www.ncbi.nlm.nih.gov/pubmed/33704674?tool=bestpractice.com
Treatment should be continued for 6 months in patients with recurrent disease. A longer duration of therapy can be considered in resistant cases. C-reactive protein (CRP) levels should be used to guide therapy and response. Once the CRP has normalized, drug therapy can be tapered gradually according to symptoms and the CRP level.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
While tapering the dose is not mandatory, it can be considered in the last few weeks of treatment to prevent persistence of symptoms and recurrence.
Before commencing treatment, a baseline complete blood count (CBC) is indicated as colchicine may cause neutropenia and bone marrow suppression. Caution should be exercised in renal and hepatic impairment as its use may be contraindicated in patients on certain medications.
Primary options
colchicine: <70 kg body weight: 0.6 mg orally once daily; ≥70 kg body weight: 0.6 mg orally twice daily
exercise restriction
Treatment recommended for ALL patients in selected patient group
Exercise should be restricted until chest pain resolves and inflammatory markers have normalized.[55]Kim JH, Baggish AL, Levine BD, et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2025 Feb 20 [Epub ahead of print]. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001297 http://www.ncbi.nlm.nih.gov/pubmed/39973614?tool=bestpractice.com A minimum of 3 months is often considered appropriate (and recommended for patients involved in competitive sports), but shorter periods of restriction may be considered depending on patient and disease characteristics (e.g., nonathletes and/or mild clinical picture).[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [56]Pelliccia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2019 Jan 1;40(1):19-33. https://academic.oup.com/eurheartj/article/40/1/19/5248228 http://www.ncbi.nlm.nih.gov/pubmed/30561613?tool=bestpractice.com
immunosuppressant
Third-line therapies in recurrent disease are immunosuppressants, including intravenous immunoglobulin (IVIG), interleukin-1 inhibitors (e.g., anakinra, and rilonacept), and azathioprine. These therapies should be used in consultation with a rheumatologist.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [20]Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015 Oct 13;314(14):1498-506. https://iris.unito.it/handle/2318/1576078#.XAFHbdv7S70 http://www.ncbi.nlm.nih.gov/pubmed/26461998?tool=bestpractice.com [57]Galluzzo A, Imazio M. Advances in medical therapy for pericardial diseases. Expert Rev Cardiovasc Ther. 2018 Sep;16(9):635-43. http://www.ncbi.nlm.nih.gov/pubmed/30103638?tool=bestpractice.com [68]Imazio M, Lazaros G, Gattorno M, et al. Anti-interleukin-1 agents for pericarditis: a primer for cardiologists. Eur Heart J. 2022 Aug 14;43(31):2946-57. https://academic.oup.com/eurheartj/article/43/31/2946/6370991 http://www.ncbi.nlm.nih.gov/pubmed/34528670?tool=bestpractice.com [69]Vianello F, Cinetto F, Cavraro M, et al. Azathioprine in isolated recurrent pericarditis: a single centre experience. Int J Cardiol. 2011 Mar 17;147(3):477-8. http://www.ncbi.nlm.nih.gov/pubmed/21296434?tool=bestpractice.com [70]Imazio M, Lazaros G, Picardi E, et al. Intravenous human immunoglobulins for refractory recurrent pericarditis: a systematic review of all published cases. J Cardiovasc Med (Hagerstown). 2016 Apr;17(4):263-9. http://www.ncbi.nlm.nih.gov/pubmed/26090917?tool=bestpractice.com [71]Emmi G, Urban ML, Imazio M, et al. Use of interleukin-1 blockers in pericardial and cardiovascular diseases. Curr Cardiol Rep. 2018 Jun 14;20(8):61. http://www.ncbi.nlm.nih.gov/pubmed/29904899?tool=bestpractice.com
Primary options
azathioprine: consult specialist for guidance on dose
OR
rilonacept: consult specialist for guidance on dose
OR
anakinra: consult specialist for guidance on dose
OR
immune globulin (human): consult specialist for guidance on dose
exercise restriction
Treatment recommended for ALL patients in selected patient group
Exercise should be restricted until chest pain resolves and inflammatory markers have normalized.[55]Kim JH, Baggish AL, Levine BD, et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2025 Feb 20 [Epub ahead of print]. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001297 http://www.ncbi.nlm.nih.gov/pubmed/39973614?tool=bestpractice.com A minimum of 3 months is often considered appropriate (and recommended for patients involved in competitive sports), but shorter periods of restriction may be considered depending on patient and disease characteristics (e.g., nonathletes and/or mild clinical picture).[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [56]Pelliccia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2019 Jan 1;40(1):19-33. https://academic.oup.com/eurheartj/article/40/1/19/5248228 http://www.ncbi.nlm.nih.gov/pubmed/30561613?tool=bestpractice.com
pericardiectomy
Patients with persistent symptomatic recurrence refractory to all medical treatment can be considered for surgical management with pericardiectomy.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64.
http://eurheartj.oxfordjournals.org/content/36/42/2921.long
http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: Pericardectomy in a 56-year-old male patient with idiopathic calcific constrictive pericarditis. The pericardium is thickened and calcifiedPatanwala I, Crilley J, Trewby PN. BMJ Case Reports 2009; doi:10.1136/bcr.06.2008.0015 [Citation ends].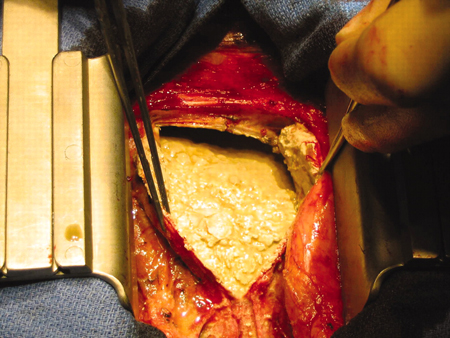
In patients with tuberculous pericarditis, pericardiectomy is reserved for those with recurrent effusions or evidence of constrictive physiology despite medical therapy.[2]Imazio M, Brucato A, Mayosi BM, et al. Medical therapy of pericardial diseases: part II: Noninfectious pericarditis, pericardial effusion and constrictive pericarditis. J Cardiovasc Med (Hagerstown). 2010 Nov;11(11):785-94. http://www.ncbi.nlm.nih.gov/pubmed/20925146?tool=bestpractice.com It is particularly recommended if the patient’s condition is not improving or is deteriorating after 4 to 8 weeks of antituberculosis therapy.[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com Pericardiectomy may also be necessary for treatment of recurrent nontuberculous pericarditis refractory to standard therapies, where constriction is present (e.g., following cardiac surgery or radiation therapy, or idiopathic constrictive pericarditis).[42]Kumar S, Khubber S, Reyaldeen R, et al. Advances in imaging and targeted therapies for recurrent pericarditis: a review. JAMA Cardiol. 2022 Sep 1;7(9):975-85. http://www.ncbi.nlm.nih.gov/pubmed/35976625?tool=bestpractice.com [73]Tzani A, Doulamis IP, Tzoumas A, et al. Meta-analysis of population characteristics and outcomes of patients undergoing pericardiectomy for constrictive pericarditis. Am J Cardiol. 2021 May 1;146:120-7. http://www.ncbi.nlm.nih.gov/pubmed/33539860?tool=bestpractice.com
exercise restriction
Treatment recommended for ALL patients in selected patient group
Exercise should be restricted until chest pain resolves and inflammatory markers have normalized.[55]Kim JH, Baggish AL, Levine BD, et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2025 Feb 20 [Epub ahead of print]. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001297 http://www.ncbi.nlm.nih.gov/pubmed/39973614?tool=bestpractice.com A minimum of 3 months is often considered appropriate (and recommended for patients involved in competitive sports), but shorter periods of restriction may be considered depending on patient and disease characteristics (e.g., nonathletes and/or mild clinical picture).[1]Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015 Nov 7;36(42):2921-64. http://eurheartj.oxfordjournals.org/content/36/42/2921.long http://www.ncbi.nlm.nih.gov/pubmed/26320112?tool=bestpractice.com [14]Little WC, Freeman GL. Pericardial disease. Circulation. 2006 Mar 28;113(12):1622-32. http://circ.ahajournals.org/cgi/content/full/113/12/1622 http://www.ncbi.nlm.nih.gov/pubmed/16567581?tool=bestpractice.com [37]Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010 Feb 23;121(7):916-28. http://www.ncbi.nlm.nih.gov/pubmed/20177006?tool=bestpractice.com [56]Pelliccia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2019 Jan 1;40(1):19-33. https://academic.oup.com/eurheartj/article/40/1/19/5248228 http://www.ncbi.nlm.nih.gov/pubmed/30561613?tool=bestpractice.com
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer