Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
oral or intravenous fluids
Typically seen in acutely ill patients with conditions such as diarrhea and vomiting, poorly controlled diabetes mellitus, or during recovery from renal failure or obstructive uropathy.
The basic treatment strategy for all patients involves the following steps:
1. Calculating the free water deficit
2. Determining a suitable serum sodium correction rate
3. Estimating ongoing free water losses (if applicable)
4. Designing a suitable fluid repletion program that takes into account the estimated free water deficit, the desired serum sodium correction rate, and any ongoing free water losses.
Fluid quantity: calculating the free water deficit is a good starting point to determine how much fluid to give initially in order to correct the abnormal serum sodium concentration. The free water deficit does not take any ongoing fluid losses into account.
[Figure caption and citation for the preceding image starts]: Free water deficit formula. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). Na = sodiumCreated by the BMJ Knowledge Centre [Citation ends].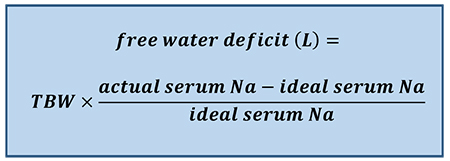
For example, an older male patient who weighs 70 kg and has a serum sodium concentration of 155 mEq/L would require 3.8 L of fluid to return his serum sodium concentration to a level of 140 mEq/L (i.e., [0.5 × 70] × [155-140/140]).
The Adrogué-Madias formula is often used in place of the free water deficit formula, as it takes into account the effect of specific fluid intake on the serum sodium concentration. It allows a prediction in the change in serum sodium concentration after the infusion of 1 L of an intravenous fluid of known sodium concentration.[Figure caption and citation for the preceding image starts]: Adrogué-Madias formula. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). Na = sodium. Sodium concentration of common fluids (per liter): normal saline (0.9%) - 154 mEq/L; lactated Ringer solution - 130 mEq/L; half-normal saline (0.45%) - 77 mEq/L; dextrose 5% in water - 0 mEq/L; enteral water - 0 mEq/LCreated by the BMJ Knowledge Centre [Citation ends].
The Adrogue-Madias formula does not take the ongoing water and electrolyte losses through urine and stool into account.[46] In addition, it is only accurate if only one liter of fluid is infused. An adapted version of the Adrogue-Madias formula, developed in 2020, can be used to determine the volume of fluid required to change the serum sodium concentration by a specific amount. [83]
[Figure caption and citation for the preceding image starts]: V = volume needed. Na = sodium. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). K = potassium. [Na]2 = the desired change in sodium concentrationCreated by the BMJ Knowledge Centre [Citation ends].
The volume calculated from this should be added to the amount of water lost via electrolyte-free water excretion during the treatment period.[Figure caption and citation for the preceding image starts]: Electrolyte-free water excretion formula. V = urine flow rate. UNa = urine concentration of sodium (mEq/L). UK = urine concentration of potassium (mEq/L). PNa = plasma concentration of sodium (mEq/L)Created by the BMJ Knowledge Centre [Citation ends].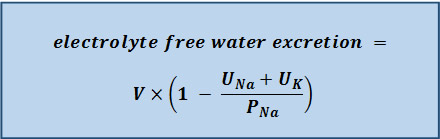
Serum sodium correction rate: patients with severe symptoms (i.e., neurologic symptoms) require more urgent treatment and more rapid correction of the sodium level for the first 2-3 hours to prevent long-term neurological complications (e.g., myelinolysis). In the first few hours, the serum sodium concentration should be lowered by 2 mEq/L/hour, followed by a correction rate of around 0.5 mEq/L/hour.[66] The acute hypernatremia correction rate should be based on careful monitoring of the symptoms/signs, volume status, serum sodium concentration, urine osmolality/electrolytes, and urine output. The aim is to lower the serum sodium level by 10 mEq/L/day in these patients if possible.[46] If the hypernatremia has developed rapidly, theoretically there is not a concern about brain edema with normalization of the elevated serum sodium.[66] However, actual data regarding the results of different treatment approaches are lacking.
A correction rate of 0.5 mEq/L/hour is commonly used in patients with chronic hypernatremia.[1] Current thinking is that sodium balance in these patients should be corrected slowly, as it is likely that the hypernatremia has developed over a long period of time, and the brain cells have had time to adapt to the high serum sodium concentration and elevated serum osmolality. Some studies have found that a more rapid correction (e.g., 3 days) may be desirable.[81][88][89] However, this approach is by no means definitive.
The rate of correction in children should not exceed 0.5 mEq/L/hour due to the high risk of seizures.[55]
Ongoing free water losses: replacing the free water deficit will usually correct the sodium abnormality in patients with hypovolemic hypernatremia.
In patients with free water losses and high electrolyte-free water excretion, replacing the free water deficit may fail to normalize the abnormal serum sodium concentration. Therefore, ongoing water losses also need to be taken into account.
In patients with ongoing urinary losses, the electrolyte-free water excretion should be calculated soon as possible.[Figure caption and citation for the preceding image starts]: Electrolyte-free water excretion formula. V = urine flow rate. UNa = urine concentration of sodium (mEq/L). UK = urine concentration of potassium (mEq/L). PNa = plasma concentration of sodium (mEq/L)Created by the BMJ Knowledge Centre [Citation ends].
The calculated amount of water should be administered in order to just maintain (or steady) the serum sodium concentration at the level from the preceding day (if a 24-hour urine sample is collected for the electrolyte-free water excretion measurement), so that the serum sodium concentration will not increase further. If urine output or the electrolyte content of the urine changes, then the electrolyte-free water excretion should be recalculated. Free water losses can also occur in patients with hypernatremia associated with inadequate free water intake or excess sodium intake; however, they are usually minimal, and replacing ongoing water losses in these patients is likely to make little, or no, difference as the electrolyte-free water excretion is usually very low.
Fluid repletion program: the initial fluid repletion program should be based on calculating the free water deficit and the desired serum sodium correction rate.
In patients with hypernatremia associated with free water losses, the amount of fluid that is actually needed to correct the abnormal serum sodium concentration is determined by adding the water deficit amount to the amount of water lost via electrolyte-free water excretion during the treatment period.
If the patient is hypovolemic and in shock, the intravascular volume should be restored urgently, usually with normal saline (0.9%), prior to free water replacement.
The initial infusion rate depends on the patient's urine output and electrolyte-free water excretion. Some physicians recommend an initial rate of approximately 3-6 mL/kg/hour (acute hypernatremia) or 1.35 mL/kg/hour (chronic hypernatremia); however, the rate of administration should be adjusted based on signs/symptoms and laboratory data.
Overall, it is common practice for half of the free water deficit to be given in the first 24 hours, with the remaining half given in the next 24 hours.[55] For example, if the total water deficit is 3.8 L, this would mean giving approximately 1.9 L of fluid per day (i.e., approximately 80 mL/hour).
Replacing free water enterally is preferred when possible. If the patient is unable to take water orally, administration via a nasogastric tube is recommended.
If enteral intake is not possible, intravenous administration is required. Fluid choices include dextrose 5% in water, balanced solutions such as lactated Ringer solution, and saline (e.g., 0.45% or 0.90%). Dextrose is preferred in most patients, while saline is generally reserved for patients with signs of severe volume depletion such as hypotension. Intravenous fluids containing sodium (which includes saline and lactated Ringer solution) should not be administered to patients with hypernatremia associated with free water losses (unless they are severely hypotensive or in shock) or accidental or iatrogenic excess intake of sodium.
In patients infused with dextrose 5% in water, the patient should be monitored for the development of hyperglycemia and associated dextrose-induced osmotic diuresis, which can worsen the hypernatremia. If hypernatremia is worsened by the patient's inability to metabolize the glucose load, a less concentrated solution of dextrose (e.g., dextrose 2.5% in water), or even pure water, may be given.
Co-existing electrolyte abnormalities (e.g., hypokalemia) should be corrected.
The regimen should always be adjusted according to patient response and serum sodium levels, rather than relying on amounts calculated from formulas.
oral or intravenous fluids
Typically occurs in a nursing home resident with dementia. Hypernatremia is relatively easy to correct in these patients by giving more free water. However, if the patient is hypovolemic and in shock, the intravascular volume should be restored urgently, usually with normal saline (0.9%), prior to free water replacement.
Once intravascular volume has been urgently restored, the basic treatment strategy for all patients involves the following steps:
1. Calculating the free water deficit
2. Determining a suitable serum sodium correction rate
3. Estimating ongoing free water losses (if applicable)
4. Designing a suitable fluid repletion program that takes into account the estimated free water deficit, the desired serum sodium correction rate, and any ongoing free water losses.
Fluid quantity: calculating the free water deficit is a good starting point to determine how much fluid to give initially in order to correct the abnormal serum sodium concentration. The free water deficit does not take any ongoing fluid losses into account.[Figure caption and citation for the preceding image starts]: Free water deficit formula. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). Na = sodiumCreated by the BMJ Knowledge Centre [Citation ends].
For example, an older male patient who weighs 70 kg and has a serum sodium concentration of 155 mEq/L would require 3.8 L of fluid to return his serum sodium concentration to a level of 140 mEq/L (i.e., [0.5 × 70] × [155-140/140]).
The Adrogué-Madias formula is often used in place of the free water deficit formula, as it takes into account the effect of specific fluid intake on the serum sodium concentration. It allows a prediction in the change in serum sodium concentration after the infusion of 1 L of an intravenous fluid of known sodium concentration.[Figure caption and citation for the preceding image starts]: Adrogué-Madias formula. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). Na = sodium. Sodium concentration of common fluids (per liter): normal saline (0.9%) - 154 mEq/L; lactated Ringer solution - 130 mEq/L; half-normal saline (0.45%) - 77 mEq/L; dextrose 5% in water - 0 mEq/L; enteral water - 0 mEq/LCreated by the BMJ Knowledge Centre [Citation ends].
The Adrogue-Madias formula does not take the ongoing water and electrolyte losses through urine and stool into account.[46] In addition, it is only accurate if only one liter of fluid is infused. An adapted version of the Adrogue-Madias formula, developed in 2020, can be used to determine the volume of fluid required to change the serum sodium concentration by a specific amount. [83]
[Figure caption and citation for the preceding image starts]: V = volume needed. Na = sodium. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). K = potassium. [Na]2 = the desired change in sodium concentrationCreated by the BMJ Knowledge Centre [Citation ends].
The volume calculated from this formula should be added to the amount of water lost via electrolyte-free water excretion during the treatment period.[Figure caption and citation for the preceding image starts]: Electrolyte-free water excretion formula. V = urine flow rate. UNa = urine concentration of sodium (mEq/L). UK = urine concentration of potassium (mEq/L). PNa = plasma concentration of sodium (mEq/L)Created by the BMJ Knowledge Centre [Citation ends].
Serum sodium correction rate: patients with severe symptoms (i.e., neurologic symptoms) require more urgent treatment and more rapid correction of the sodium level for the first 2-3 hours to prevent long-term neurologic complications (e.g., myelinolysis). In the first few hours, the serum sodium concentration should be lowered by 2 mEq/L/hour, followed by a correction rate of around 0.5 mEq/L/hour.[66] The acute hypernatremia correction rate should be based on careful monitoring of the symptoms/signs, volume status, serum sodium concentration, urine osmolality/electrolytes, and urine output. The aim is to lower the serum sodium level by 10 mEq/L/day in these patients if possible.[46] If the hypernatremia has developed rapidly, theoretically there is not a concern about brain edema with normalization of the elevated serum sodium.[66] However, actual data regarding the results of different treatment approaches are lacking. A correction rate of 0.5 mEq/L/hour is commonly used in patients with chronic hypernatremia.[1]
Current thinking is that sodium balance in these patients should be corrected slowly, as it is likely that the hypernatremia has developed over a long period of time, and the brain cells have had time to adapt to the high serum sodium concentration and elevated serum osmolality. Some studies have found that a more rapid correction (e.g., 3 days) may be desirable.[81][88][89] However, this approach is by no means definitive.
The rate of correction in children should not exceed 0.5 mEq/L/hour due to the high risk of seizures.[55]
Ongoing free water losses: replacing the free water deficit will usually correct the sodium abnormality in patients with hypovolemic hypernatremia.
In patients with free water losses and high electrolyte-free water excretion, replacing the free water deficit may fail to normalize the abnormal serum sodium concentration. Therefore, ongoing water losses also need to be taken into account.
In patients with ongoing urinary losses, calculate the electrolyte-free water excretion soon as possible.[Figure caption and citation for the preceding image starts]: Electrolyte-free water excretion formula. V = urine flow rate. UNa = urine concentration of sodium (mEq/L). UK = urine concentration of potassium (mEq/L). PNa = plasma concentration of sodium (mEq/L)Created by the BMJ Knowledge Centre [Citation ends].
The calculated amount of water should be administered in order to just maintain (or steady) the serum sodium concentration at the level from the preceding day (if a 24-hour urine sample is collected for the electrolyte-free water excretion measurement), so that the serum sodium concentration will not increase further. If urine output or the electrolyte content of the urine changes, then the electrolyte-free water excretion should be recalculated.
Free water losses can also occur in patients with hypernatremia associated with inadequate free water intake or excess sodium intake; however, they are usually minimal, and replacing ongoing water losses in these patients is likely to make little, or no, difference as the electrolyte-free water excretion is usually very low.
Fluid repletion program: the initial fluid repletion program should be based on calculating the free water deficit and the desired serum sodium correction rate.
In patients with hypernatremia associated with free water losses, the amount of fluid that is actually needed to correct the abnormal serum sodium concentration is determined by adding the water deficit amount to the amount of water lost via electrolyte-free water excretion during the treatment period.
If the patient is hypovolemic and in shock, the intravascular volume should be restored urgently, usually with normal saline (0.9%), prior to free water replacement.
The initial infusion rate depends on the patient's urine output and electrolyte-free water excretion. Some physicians recommend an initial rate of approximately 3-6 mL/kg/hour (acute hypernatremia) or 1.35 mL/kg/hour (chronic hypernatremia); however, the rate of administration should be adjusted based on signs/symptoms and laboratory data.
Overall, it is common practice for half of the free water deficit to be given in the first 24 hours, with the remaining half given in the next 24 hours.[55] For example, if the total water deficit is 3.8 L, this would mean giving approximately 1.9 L of fluid per day (i.e., approximately 80 mL/hour).
Replacing free water enterally is preferred when possible. If the patient is unable to take water orally, administration via a nasogastric tube is recommended.
If enteral intake is not possible, intravenous administration is required. Fluid choices include dextrose 5% in water, balanced solutions such as lactated Ringer solution, and saline (e.g., 0.45% or 0.90%). Dextrose is preferred in most patients, while saline is generally reserved for patients with signs of severe volume depletion such as hypotension. Intravenous fluids containing sodium (which includes saline and lactated Ringer solution) should not be administered to patients with hypernatremia associated with free water losses (unless they are severely hypotensive or in shock) or accidental or iatrogenic excess intake of sodium.
In patients infused with dextrose 5% in water, the patient should be monitored for the development of hyperglycemia and associated dextrose-induced osmotic diuresis, which can worsen the hypernatremia. If hypernatremia is worsened by the patient's inability to metabolize the glucose load, a less concentrated solution of dextrose (e.g., dextrose 2.5% in water), or even pure water, may be given.
Co-existing electrolyte abnormalities (e.g., hypokalemia) should be corrected. The regimen should always be adjusted according to patient response and serum sodium levels, rather than relying on amounts calculated from formulas.
oral or intravenous fluids
As patients are not volume depleted, they should receive only enough free water to correct the hypernatremia.
The basic treatment strategy for all patients involves the following steps:
1. Calculating the free water deficit
2. Determining a suitable serum sodium correction rate
3. Estimating ongoing free water losses (if applicable)
4. Designing a suitable fluid repletion program that takes into account the estimated free water deficit, the desired serum sodium correction rate, and any ongoing free water losses.
Fluid quantity: calculating the free water deficit is a good starting point to determine how much fluid to give initially in order to correct the abnormal serum sodium concentration. The free water deficit does not take any ongoing fluid losses into account.[Figure caption and citation for the preceding image starts]: Free water deficit formula. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). Na = sodiumCreated by the BMJ Knowledge Centre [Citation ends].
For example, an older male patient who weighs 70 kg and has a serum sodium concentration of 155 mEq/L would require 3.8 L of fluid to return his serum sodium concentration to a level of 140 mEq/L (i.e., [0.5 × 70] × [155-140/140]).
The Adrogué-Madias formula is often used in place of the free water deficit formula, as it takes into account the effect of specific fluid intake on the serum sodium concentration. It allows a prediction in the change in serum sodium concentration after the infusion of 1 L of an intravenous fluid of known sodium concentration.[Figure caption and citation for the preceding image starts]: Adrogué-Madias formula. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). Na = sodium. Sodium concentration of common fluids (per liter): normal saline (0.9%) - 154 mEq/L; lactated Ringer solution - 130 mEq/L; half-normal saline (0.45%) - 77 mEq/L; dextrose 5% in water - 0 mEq/L; enteral water - 0 mEq/LCreated by the BMJ Knowledge Centre [Citation ends].
The Adrogue-Madias formula does not take the ongoing water and electrolyte losses through urine and stool into account.[46] In addition, it is only accurate if only one liter of fluid is infused. An adapted version of the Adrogue-Madias formula, developed in 2020, can be used to determine the volume of fluid required to change the serum sodium concentration by a specific amount. [83]
[Figure caption and citation for the preceding image starts]: V = volume needed. Na = sodium. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). K = potassium. [Na]2 = the desired change in sodium concentrationCreated by the BMJ Knowledge Centre [Citation ends].
The volume calculated from this formula should be added to the amount of water lost via electrolyte-free water excretion during the treatment period.[Figure caption and citation for the preceding image starts]: Electrolyte-free water excretion formula. V = urine flow rate. UNa = urine concentration of sodium (mEq/L). UK = urine concentration of potassium (mEq/L). PNa = plasma concentration of sodium (mEq/L)Created by the BMJ Knowledge Centre [Citation ends].
Serum sodium correction rate: patients with severe symptoms (i.e., neurologic symptoms) require more urgent treatment and more rapid correction of the sodium level for the first 2-3 hours to prevent long-term neurologic complications (e.g., myelinolysis). In the first few hours, the serum sodium concentration should be lowered by 2 mEq/L/hour, followed by a correction rate of around 0.5 mEq/L/hour.[66] The acute hypernatremia correction rate should be based on careful monitoring of the symptoms/signs, volume status, serum sodium concentration, urine osmolality/electrolytes, and urine output. The aim is to lower the serum sodium level by 10 mEq/L/day in these patients if possible.[46] If the hypernatremia has developed rapidly, theoretically there is not a concern about brain edema with normalization of the elevated serum sodium.[66] However, actual data regarding the results of different treatment approaches are lacking.
A correction rate of 0.5 mEq/L/hour is commonly used in patients with chronic hypernatremia.[1] Current thinking is that sodium balance in these patients should be corrected slowly, as it is likely that the hypernatremia has developed over a long period of time, and the brain cells have had time to adapt to the high serum sodium concentration and elevated serum osmolality. Some studies have found that a more rapid correction (e.g., 3 days) may be desirable.[81][88][89] However, this approach is by no means definitive.
The rate of correction in children should not exceed 0.5 mEq/L/hour due to the high risk of seizures.[55]
Ongoing free water losses: replacing the free water deficit will usually correct the sodium abnormality in patients with hypovolemic hypernatremia.
In patients with free water losses and high electrolyte-free water excretion, replacing the free water deficit may fail to normalize the abnormal serum sodium concentration. Therefore, ongoing water losses may also need to be taken into account.
In patients with ongoing urinary losses, calculate the electrolyte-free water excretion soon as possible.[Figure caption and citation for the preceding image starts]: Electrolyte-free water excretion formula. V = urine flow rate. UNa = urine concentration of sodium (mEq/L). UK = urine concentration of potassium (mEq/L). PNa = plasma concentration of sodium (mEq/L)Created by the BMJ Knowledge Centre [Citation ends].
The calculated amount of water should be administered in order to just maintain (or steady) the serum sodium concentration at the level from the preceding day (if a 24-hour urine sample is collected for the electrolyte-free water excretion measurement), so that the serum sodium concentration will not increase further. If urine output or the electrolyte content of the urine changes, then the electrolyte-free water excretion should be recalculated.
Free water losses can also occur in patients with hypernatremia associated with inadequate free water intake or excess sodium intake; however, they are usually minimal, and replacing ongoing water losses in these patients is likely to make little, or no difference as the electrolyte-free water excretion is usually very low.
Fluid repletion program: the initial fluid repletion program should be based on calculating the free water deficit and the desired serum sodium correction rate.
In patients with hypernatremia associated with free water losses, the amount of fluid that is actually needed to correct the abnormal serum sodium concentration is determined by adding the water deficit amount to the amount of water lost via electrolyte-free water excretion during the treatment period.
If the patient is hypovolemic and in shock, the intravascular volume should be restored urgently, usually with normal saline (0.9%), prior to free water replacement.
The initial infusion rate depends on the patient's urine output and electrolyte-free water excretion. Some physicians recommend an initial rate of approximately 3-6 mL/kg/hour (acute hypernatremia) or 1.35 mL/kg/hour (chronic hypernatremia); however, the rate of administration should be adjusted based on signs/symptoms and laboratory data.
Overall, it is common practice for half of the free water deficit to be given in the first 24 hours, with the remaining half given in the next 24 hours.[55] For example, if the total water deficit is 3.8 L, this would mean giving approximately 1.9 L of fluid per day (i.e., approximately 80 mL/hour).
Replacing free water enterally is preferred when possible. If the patient is unable to take water orally, administration via a nasogastric tube is recommended.
If enteral intake is not possible, intravenous administration is required. Fluid choices include dextrose 5% in water, balanced solutions such as lactated Ringer solution, and saline (e.g., 0.45% or 0.90%). Dextrose is preferred in most patients, while saline is generally reserved for patients with signs of severe volume depletion such as hypotension. Intravenous fluids containing sodium (which includes saline and lactated Ringer solution) should not be administered to patients with hypernatremia associated with free water losses (unless they are severely hypotensive or in shock) or accidental or iatrogenic excess intake of sodium.
In patients infused with dextrose 5% in water, the patient should be monitored for the development of hyperglycemia and associated dextrose-induced osmotic diuresis, which can worsen the hypernatremia. If hypernatremia is worsened by the patient's inability to metabolize the glucose load, a less concentrated solution of dextrose (e.g., dextrose 2.5% in water), or even pure water, may be given.
Co-existing electrolyte abnormalities (e.g., hypokalemia) should be corrected.
The regimen should always be adjusted according to patient response and serum sodium levels, rather than relying on amounts calculated from formulas.
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer