Complications
If hypernatremia is corrected too quickly in the setting of chronic hypernatremia, the lowering of the serum osmolality can lead to water movement into the brain cells causing brain edema.
CT scan of the brain shows diffuse sulcal effacement and slight blurring of grey-white differentiation consistent with global cerebral edema.[Figure caption and citation for the preceding image starts]: CT brain showing diffuse sulcal effacement and slight blurring of grey-white differentiation consistent with global cerebral edema. There is no evidence of herniationDr Hari Trivedi, Department of Radiology, San Francisco General Hospital, University of California; used with permission [Citation ends].
May develop due to rapid administration of dextrose-containing fluids.
More likely to occur in patients with diabetes, those with physiologic stress, or when high infusion rates are used.
Patients should be monitored for the development of hyperglycemia and associated dextrose-induced osmotic diuresis, which can worsen the hypernatremia.
If hypernatremia is worsened by the patient’s inability to metabolize the glucose load, a less concentrated solution of dextrose (e.g., dextrose 2.5% in water), or even pure water, may be given.
Myelinolysis (also known as osmotic demyelination syndrome) has been described rarely in patients with hypernatremia (it is more common in patients with rapid correction of hyponatremia).[66][117][118][119]
Hypernatremia-induced osmotic demyelination can lead to permanent neurological dysfunction.[118]
Brain MRI shows a symmetric central pontine lesion with trident shape and areas of restricted diffusion.[Figure caption and citation for the preceding image starts]: Brain MRI showing a symmetric central pontine lesion (arrows), sparing the peripheral fibers, with a typical trident shape and areas of restricted diffusion. Suggests osmotic demyelination syndrome. Note the symmetric thalamic lesions (open arrows) in images B and CBMJ Case Reports 2012, doi: 10.1136/bcr:11.2011.5198 [Citation ends].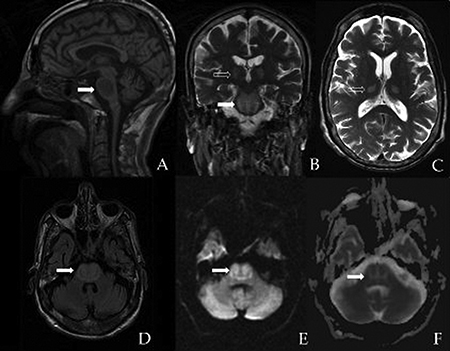
Use of this content is subject to our disclaimer