Approach
Treatment should be directed at addressing the underlying cause (e.g., stop offending medication, treat fever, relieve urinary obstruction, give insulin, discontinue sodium sources), as well as replacing any free water deficit and ongoing fluid losses, while monitoring serum sodium concentration to ensure levels are returning to the correct range at the desired rate. There is no consensus on the ideal correction rate. It is important not to correct the serum sodium concentration too rapidly because of the risk of cerebral edema; conversely, one study suggested that correcting the serum sodium concentration too slowly may also be harmful.[81] One systematic review concluded that there is an absence of good-quality evidence (randomized- or observational-controlled trials) for active correction of hypernatremia in resuscitated patients recovering from critical illness.[82]
Treatment strategy
The basic treatment strategy for all patients involves the following steps:
Calculating the free water deficit
Determining a suitable serum sodium correction rate
Estimating ongoing free water losses (if applicable)
Designing a suitable fluid repletion program that takes into account the estimated free water deficit, the desired serum sodium correction rate, and any ongoing free water losses.
More specific treatment is guided by the presence of signs/symptoms, severity of symptoms, time of onset, and volume status of the patient.
Severe or acute hypernatremia should always be treated in hospital; however, mild or chronic hypernatremia can be managed in the outpatient setting.
Calculating the free water deficit
Calculating the free water deficit is a good starting point to determine how much fluid to give initially in order to correct the abnormal serum sodium concentration. The free water deficit does not take any ongoing fluid losses into account.[5][Figure caption and citation for the preceding image starts]: Free water deficit formula. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). Na = sodiumCreated by the BMJ Knowledge Centre [Citation ends].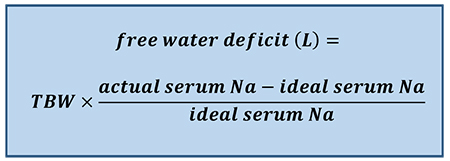
For example, an older male patient who weighs 70 kg and has a serum sodium concentration of 155 mEq/L would require 3.8 L of fluid to return his serum sodium concentration to a level of 140 mEq/L [i.e., (0.5 × 70) × (155-140/140)].
The Adrogué-Madias formula is often used in place of the free water deficit formula as it takes into account the effect of specific fluid intake on the serum sodium concentration. It allows a prediction in the change in serum sodium concentration after the infusion of 1 L of an intravenous fluid of known sodium concentration. [Figure caption and citation for the preceding image starts]: Adrogué-Madias formula. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). Na = sodium. Sodium concentration of common fluids (per liter): normal saline (0.9%) - 154 mEq/L; lactated Ringer solution - 130 mEq/L; half-normal saline (0.45%) - 77 mEq/L; dextrose 5% in water - 0 mEq/L; enteral water - 0 mEq/LCreated by the BMJ Knowledge Centre [Citation ends].
The Adrogué-Madias formula does not take the ongoing water and electrolyte losses through urine and stool into account.[46] In addition, the formula is only accurate if only one liter of fluid is infused. An adapted version of the Adrogué-Madias formula, developed in 2020, can be used to determine the volume of fluid required to change the serum sodium concentration by a specified amount. [83]
[Figure caption and citation for the preceding image starts]: V = volume needed. Na = sodium. TBW (total body water) = patient body weight (kg) x 0.5 (women/older men) or 0.6 (young men or children) or 0.4 (dehydrated patients). K = potassium. [Na]2 = the desired change in sodium concentrationCreated by the BMJ Knowledge Centre [Citation ends].
The Kurtz-Nguyen formulas have been published in various papers.[84][85][86][87] However, they are complicated and are more useful in understanding sodium disorders than they are for managing patients in clinical practice.
Determining a suitable serum sodium correction rate
Patients with severe symptoms (i.e., neurologic symptoms) require more urgent treatment and more rapid correction of the sodium level for the first 2-3 hours to prevent long-term neurologic complications (e.g., myelinolysis). In the first few hours, the serum sodium concentration should be lowered by 2 mEq/L/hour, followed by a correction rate of around 0.5 mEq/L/hour.[66] The acute hypernatremia correction rate should be based on careful monitoring of the symptoms/signs, volume status, serum sodium concentration, urine osmolality/electrolytes, and urine output. The aim is to lower the serum sodium level by 10 mEq/L/day in these patients if possible.[46] One study advocated normalizing the serum sodium concentration in less than 24 hours in cases of acute hypernatremia.[4] If the hypernatremia has developed rapidly, theoretically there is not a concern about brain edema with normalization of the elevated serum sodium.[66] However, actual data regarding the results of different treatment approaches are lacking.
A correction rate of 0.5 mEq/L/hour is commonly used in patients with chronic hypernatremia.[1] Current thinking is that sodium balance in these patients should be corrected slowly, as it is likely that the hypernatremia has developed over days, weeks, or even months and the brain cells have had time to adapt to the high serum sodium concentration and elevated serum osmolality. Some studies have found that a more rapid correction (e.g., 3 days) may be desirable.[81][88][89] However, this approach is by no means definitive.
The rate of correction in children should not exceed 0.5 mEq/L/hour due to the high risk of seizures.[55]
Estimating ongoing free water losses
Replacing the free water deficit will usually correct the sodium abnormality in patients with hypovolemic hypernatremia.
In patients with free water losses and high electrolyte-free water excretion, replacing the free water deficit may fail to normalize the abnormal serum sodium concentration. Therefore, ongoing water losses also need to be taken into account.
In patients with ongoing urinary losses, the electrolyte-free water excretion should be calculated as soon as possible.[Figure caption and citation for the preceding image starts]: Electrolyte-free water excretion formula. V = urine flow rate. UNa = urine concentration of sodium (mEq/L). UK = urine concentration of potassium (mEq/L). PNa = plasma concentration of sodium (mEq/L)Created by the BMJ Knowledge Centre [Citation ends].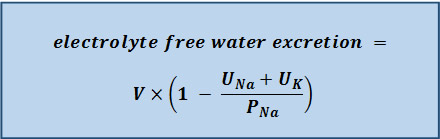
The calculated amount of water should be administered in order to just maintain (or steady) the serum sodium concentration at the level from the preceding day (if a 24-hour urine sample is collected for the electrolyte-free water excretion measurement), so that the serum sodium concentration will not increase further. If urine output or the electrolyte content of the urine changes, then the electrolyte-free water excretion should be recalculated.
Free water losses can also occur in patients with hypernatremia associated with inadequate free water intake or excess sodium intake; however, they are usually minimal, and replacing ongoing water losses in these patients is likely to make little, or no, difference as the electrolyte-free water excretion is usually very low.
Designing a fluid repletion program
The initial fluid repletion program should be based on calculating the free water deficit and the desired serum sodium correction rate. In patients with hypernatremia associated with free water losses, the amount of fluid that is actually needed to correct the abnormal serum sodium concentration is determined by adding the water deficit amount to the amount of water lost via electrolyte-free water excretion during the treatment period.
If the patient is hypovolemic and in shock, the intravascular volume should be restored urgently, usually with normal saline (0.9%), prior to free water replacement.
The initial infusion rate depends on the patient's urine output and electrolyte-free water excretion. Some physicians recommend an initial rate of approximately 3-6 mL/kg/hour (acute hypernatremia) or 1.35 mL/kg/hour (chronic hypernatremia); however, the rate of administration should be adjusted based on signs/symptoms and laboratory data.
Overall, it is common practice for half of the free water deficit to be given in the first 24 hours, with the remaining half given in the next 24 hours.[55] For example, if the total water deficit is 3.8 L, this would mean giving approximately 1.9 L of fluid per day (i.e., approximately 80 mL/hour).
Replacing free water enterally is preferred when possible. If the patient is unable to take water orally, administration via a nasogastric tube is recommended.
If enteral intake is not possible, intravenous administration is required. Fluid choices include dextrose 5% in water, balanced solutions such as lactated Ringer solution, and saline (e.g., 0.45% or 0.9%). Dextrose is preferred in most patients, while saline is generally reserved for patients with signs of severe volume depletion such as hypotension. Intravenous fluids containing sodium (which includes saline and lactated Ringer solution) should not be administered to patients with hypernatremia associated with free water losses (unless they are severely hypotensive or in shock) or accidental or iatrogenic excess intake of sodium.
In patients infused with dextrose 5% in water, the patient should be monitored for the development of hyperglycemia and associated dextrose-induced osmotic diuresis, which can worsen the hypernatremia. If hypernatremia is worsened by the patient’s inability to metabolize the glucose load, a less concentrated solution of dextrose (e.g., dextrose 2.5% in water), or even pure water, may be given.
Co-existing electrolyte abnormalities (e.g., hypokalemia) should be corrected.
The regimen should always be adjusted according to patient response and serum sodium levels, rather than relying on amounts calculated from formulas.
Monitoring
The above formulas can help to determine the approximate amount of water that is needed to correct the serum sodium abnormalities; however, they are not exact, and frequent measurement of the serum sodium concentration (e.g., every 1-2 hours for acute hypernatremia or every 4-6 hours for chronic hypernatremia until stable, then every 12-24 hours) is necessary to make sure that levels are returning to the correct range at the desired rate.
Other parameters that should be monitored throughout the treatment period include:
Urine sodium and potassium concentration
Urine osmolality
Urine output.
This information helps determine the amount of water needed to replace the ongoing losses.
Serum electrolytes should also be monitored to assess for electrolyte imbalances (e.g., hypokalemia), and serum glucose to assess for treatment-related hyperglycemia (if dextrose-containing solutions are used).
Diabetes insipidus
Central diabetes insipidus:
Treatment of choice is desmopressin (DDAVP), a synthetic analog of vasopressin (also known as arginine vasopressin [AVP] or antidiuretic hormone [ADH]). Desmopressin reduces urinary losses (and electrolyte-free water excretion), and can be administered orally, intranasally, or parenterally.[90] Treatment should be started with a low dose and increased gradually according to response.
Fluids should also be given. Electrolyte-free water excretion must be replaced; however, desmopressin therapy is usually sufficient to stop ongoing losses. Previous losses need to be replaced.
Hypernatremia in the setting of central diabetes insipidus should be treated as a medical emergency and managed in a high-dependency area. In patients who are intravascularly depleted, intravenous rehydration with 0.9% sodium chloride should precede consideration of free water administration.[90]
Nephrogenic diabetes insipidus:
Patients do not respond to desmopressin and will, therefore, require large amounts of water just to keep their serum sodium concentration the same, and even more water to correct the hypernatremia. The route of administration depends on the clinical status of the patient. If they have altered mental status, the intravenous route is preferred. If they are relatively well and able to drink water, the oral route is preferred.
Adding the electrolyte-free water excretion to the free water deficit will help in working out a starting point of how much water to give.
Thiazide diuretics interfere with the diluting ability of the kidney and cause mild volume depletion and increased proximal reabsorption of sodium and water. As such, they are helpful in decreasing the urine output in patients with nephrogenic diabetes insipidus.
See Diabetes insipidus.
Accidental or iatrogenic excess intake of sodium
In addition to the general treatment principles above, loop diuretics can be used as an adjunctive treatment in patients with hypernatremia associated with excess salt intake and fluid overload to increase renal sodium excretion; however, fluid losses during therapy should be replaced with free water. Loop diuretics do not correct the hypernatremia (if anything, they can make it worse); they are used to decrease the sodium overload in these patients.
Renal replacement therapy
These methods are used in patients with preexisting, advanced renal failure or those with fluid overload or sodium overload.
With continuous slow administration, and adjustments of the sodium level in the dialysate or in the replacement fluid, continuous renal replacement therapies have resulted in good outcomes.[91][92][93][94][95][96][97][98][99] Use of slow dialysis, in the form of continuous dialysis or sustained low-efficiency dialysis, has only been reported in patients with acute hypernatremia.
Hemodialysis and hemofiltration may correct the sodium level too quickly. One study found that correcting the serum sodium concentration by >1 mEq/L/hour in acute severe hypernatremia was associated with higher mortality.[100] Adverse outcomes may be avoided by appropriate increases in the sodium level of the dialysate or replacement fluid, and reduction of the rate of correction by using slower blood and dialysate flows and lower-efficiency dialyzers (e.g., sustained low-efficiency dialysis).
Peritoneal dialysis using a low-sodium dialysate has been found to be effective in treating hypernatremia due to renal failure.[101]
Use of this content is subject to our disclaimer