Etiology
Etiology is associated with human herpesvirus-8 (HHV-8, also known as Kaposi sarcoma-associated herpesvirus [KSHV]) infection.[1]
HHV-8 infection, in combination with impaired host immunity, causes KS. While HIV-associated KS and iatrogenic KS are associated with distinct immunodeficiency, impaired immune function in classic KS and endemic KS is less clearly characterized.[4]
Pathophysiology
Although it is not specific to KS, human herpesvirus-8 (HHV-8) infection is thought to be necessary for the development of lesions. Lesions of all epidemiologic forms are histologically similar. Morphologically they are composed of spindle-shaped, vasoformative tumor cells, abnormal vessels, and chronic inflammatory cells.[22] The lesional cells in KS express latency-associated nuclear antigen-1 (LANA-1) of HHV-8, which may be detected using immunohistochemistry.
Lesions evolve from an early patch, to a plaque, and later to tumor nodules. Regression of lesions may occur spontaneously (although this is rare), after antiretroviral therapy (ART), or following withdrawal of immunosuppressive drugs. Flare (exacerbation) of lesions can occur with immune reconstitution inflammatory syndrome (IRIS) following ART in AIDS patients, after corticosteroids, and with rituximab therapy.[23][24][25] HIV coinfection is thought to be synergistic, resulting in more aggressive and widespread KS disease. [Figure caption and citation for the preceding image starts]: Photomicrograph of the histopathology of Kaposi sarcoma showing fascicles of vasoformative spindle-shaped tumor cells (hematoxylin and eosin stain)From the collection of Dr Liron Pantanowitz; used with permission [Citation ends].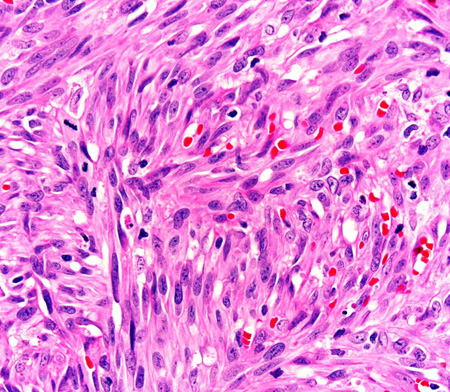
Classification
Use of this content is subject to our disclaimer