Aetiology
Repetitive motion of the wrist, elbow, and forearm over prolonged periods of time prompts the development of both medial and lateral epicondylitis.[1] Many recreational and occupational activities have been implicated.[4][10][11][12][13][14][15][16][17][18][19][20] These include:
Tennis
Fencing
Golf
Rowing
Baseball (pitching)
Hammering
Typing
Meat-cutting
Plumbing
Painting.
Other contributing factors include:
Poor mechanics and improper equipment (e.g., performing a back-handed swing with either an extended elbow or flexed wrist, or using an oversized racket handle).[21][22][23][24]
Inadequate physical conditioning and playing on hard (fast) surfaces, leading to early fatigue with resultant worsening technique.[4][5]
Less commonly, decreased elbow proprioception (e.g., secondary to a pre-existing neurological condition or previous elbow injury). This has been found in a group of patients with lateral epicondylitis, thereby altering their elbow flexion and extension mechanics.[23]
Pathophysiology
Microtears in the muscles originating at the elbow are the probable pathological process resulting in the symptoms of both lateral and medial epicondylitis.[3]
In lateral epicondylitis, lesions commonly occur within the origin of the extensor carpi radialis brevis, but may also originate in the extensor digitorum communis or extensor carpi radialis longus tendon.[4][25][Figure caption and citation for the preceding image starts]: Coronal MRI and axial MRI in the same patient, showing high signal in extensor carpi radialis brevisFrom the collection of Daniel J. Solomon, Naval Medical Center San Diego, CA; used with permission [Citation ends]. In medial epicondylitis, lesions may occur in the pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris.[9][26][Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: probe placed on area of degenerative tendon showing loss of normal tendon appearanceFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
In medial epicondylitis, lesions may occur in the pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris.[9][26][Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: probe placed on area of degenerative tendon showing loss of normal tendon appearanceFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].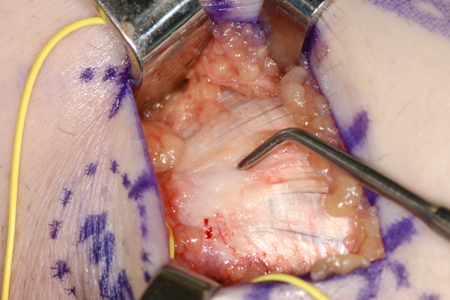 The muscular microtears are generally thought to occur as the result of repetitive valgus forces to the elbow, causing stress and muscle injury at the site of origin.[22][27]
The muscular microtears are generally thought to occur as the result of repetitive valgus forces to the elbow, causing stress and muscle injury at the site of origin.[22][27]
Areas of hypovascularity, proximal and distal to the lateral epicondyle, have been identified by histological studies and power-Doppler ultrasound.[28][29] These areas of hypovascularity are closely related to regions within the common extensor mass of the forearm with a high proportion of microtears, potentially making this tissue more susceptible to damage.
After injury, damaged tendons are characterised by signs of oedema, with disruption of the normal parallel orientation of the collagen fibres.[12] An invasion of fibroblasts and vascular granulation, known as angiofibroblastic hyperplasia, occurring within epicondylitis tissue, has been described.[30][31] Further histological assessment of the common extensor mass tendon in patients with lateral epicondylitis has demonstrated a loss of tenocytes with calcific replacement, indicating that tissue remodelling has occurred after insult.[32][Figure caption and citation for the preceding image starts]: Coronal MRI and axial MRI in the same patient, showing high signal in extensor carpi radialis brevisFrom the collection of Daniel J. Solomon, Naval Medical Center San Diego, CA; used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: pick-ups lifting off area of degenerative tendon after elliptical incision to excise this areaFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].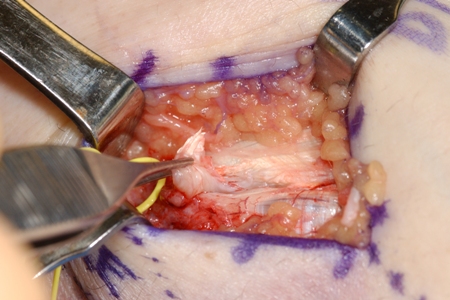 [Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: probe placed on area of degenerative tendon showing loss of normal tendon appearanceFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: probe placed on area of degenerative tendon showing loss of normal tendon appearanceFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
Use of this content is subject to our disclaimer