Aetiology
Human pituitary adenomas, including prolactinomas, are monoclonal in origin.[3] This suggests that pituitary tumours arise from the proliferation of single, mutated pituitary cells, where somatic cell mutations stimulate cellular growth rate. The majority of prolactinomas occur sporadically. A small percentage of patients may have multiple endocrine neoplasia syndrome type 1 (MEN-1) or familial isolated pituitary adenoma (FIPA). In studies of FIPA patients, prolactinomas associated with aryl hydrocarbon receptor-interacting protein (AIP) gene mutations were large, occurred at a young age (<30 years), were invasive, had suprasellar extension, and were resistant to dopamine agonist treatment.[4][5] Consideration should be given to screening young patients (<40 years) presenting with large prolactinomas for AIP gene mutations and MEN-1.[6][7]
Pathophysiology
Prolactinomas are anterior pituitary lactotroph tumours. Hypersecretion of prolactin causes secondary hypogonadism via its inhibitory effects on gonadotrophin-releasing hormone and pituitary gonadotrophins. Dopamine is transported from the hypothalamus to the anterior pituitary by hypophysial portal vessels, where it inhibits prolactin secretion via dopamine receptors expressed by lactotrophs. Therefore, disruption of dopamine secretion or transport to the portal vessels can lead to hyperprolactinaemia.
Classification
Classification according to tumour size
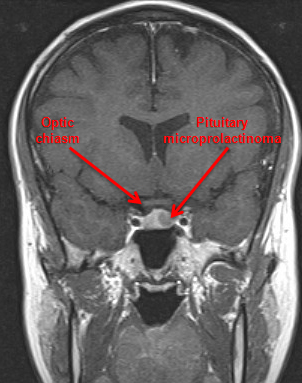
Microadenomas:
Small, intrasellar tumours, <10 mm in diameter
Rarely increase in size
Most common type in women.
Macroadenomas:
Larger tumours, >10 mm in diameter
Usually locally invasive into the suprasellar or parasellar regions
Sometimes associated with aggressive compression of vital structures
Men and post-menopausal women more commonly present with large and invasive adenomas, occasionally giant tumours (4 cm or greater)
Almost invariably benign (malignant prolactinomas that metastasise outside the pituitary sella are very rare).[Figure caption and citation for the preceding image starts]: Gadolinium-enhanced magnetic resonance imaging showing a left-sided 7 mm pituitary microprolactinomaFrom the collection of Dr Ilan Shimon [Citation ends].
 [Figure caption and citation for the preceding image starts]: Gadolinium-enhanced magnetic resonance imaging showing a large pituitary macroadenoma in a 45-year-old man with hyperprolactinaemiaFrom the collection of Dr Ilan Shimon [Citation ends].
[Figure caption and citation for the preceding image starts]: Gadolinium-enhanced magnetic resonance imaging showing a large pituitary macroadenoma in a 45-year-old man with hyperprolactinaemiaFrom the collection of Dr Ilan Shimon [Citation ends].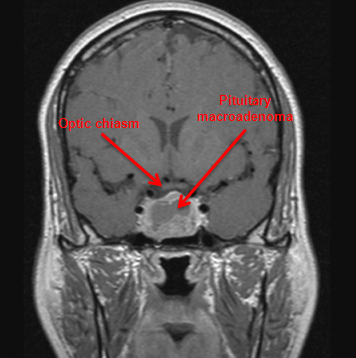
Use of this content is subject to our disclaimer