Investigations
1st investigations to order
biopsy and histopathological assessment
Test
Skin biopsy confirms the diagnosis and provides prognostic information. Any non-tender cutaneous nodule with non-specific morphology that is fast growing should be biopsied rather than monitored.[7]
A punch, incisional, or excisional biopsy should be performed on any suspicious lesion.[3][7][39][43] The most appropriate method will depend on the size and location of the tumour.
Immunohistochemistry (IHC) must be used in conjunction with haematoxylin and eosin (H&E) for confirmation of the diagnosis and to rule out histological mimics (most notably, other small cell tumours, including basal cell carcinoma, small cell lung cancer, and small cell melanoma).[3][7][29][39][43]
Cytokeratin 20 (CK20) positivity and thyroid transcription factor (TTF-1) negativity is characteristic of MCC, although variations are reported. MCC also stains positive for epithelial markers AE1/AE3, and CAM5.2, and for neuroendocrine markers such as neuron-specific enolase (NSE), synaptophysin, CD56, and chromogranin A. MCPyV large T expression is a specific but not wholly sensitive marker.
In addition to TTF-1 negativity, MCC is negative for S-100 and HMB-45, cytokeratin 7, carcinoembryonic antigen (CEA), leukocyte common antigen, and lymphoma-specific lymphocytic markers.
[Figure caption and citation for the preceding image starts]: Histological features of MCC from biopsy of a primary tumour. Image B shows small round blue cells and image C shows characteristic nuclei, finely granular and dusty 'salt and pepper' chromatin, and abundant mitotic figuresMauzo SH et al. J Clin Pathol 2016; 69: 382-90; used with permission [Citation ends].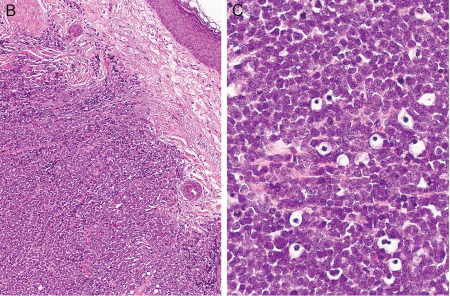
Result
H&E: dermally-based tumour of small round blue cells with hyperchromatic nuclei, 'salt and pepper' chromatin pattern, and high mitotic activity; confirmatory IHC stains distinguish MCC from histopathological mimics
dermoscopy
Test
Dermoscopy can be useful in raising suspicion of malignancy, although the dermoscopic pattern of MCC is non-specific.[7] It can be particularly helpful for patients with multiple skin lesions as MCC can sometimes be contiguous to, or intermingled with, other skin cancers that can be more easily identified with dermoscopy.[19]
Result
may show prominent red or milky-red background colour or smaller clods of milky-red areas, polymorphous vessels, and white areas
Investigations to consider
lymph node ultrasound
Test
Recommended for patients with clinical stage I or II disease.[19]
Result
may show regional disease
whole-body PET scan
Test
After confirmation of the diagnosis of MCC, imaging is recommended for all patients to evaluate for regional lymph node metastases and distant disease and for staging of the disease.[3][19][44]
Data indicate that whole-body fluorodeoxyglucose-positron emission tomography (FDG-PET) with fused axial imaging is the most reliable method for detecting occult metastatic MCC at baseline.[49][50] It is therefore recommended as the preferred cross-sectional imaging modality, if available, to assess local and distant disease.[3][19]
Result
may show metastases
CT scan with contrast chest/abdomen/pelvis (± neck)
brain MRI
Test
MRI of the brain (with or without contrast) is recommended if there is clinical suspicion of brain metastases (e.g., neurological symptoms).[3]
Result
may show metastases
fine needle aspiration or core biopsy
sentinel lymph node biopsy (SLNB)
Test
In patients presenting without detectable metastatic disease, use SLNB to identify subclinical metastatic disease in the regional nodal basin.[33][34][35][42][44][51]
SLNB should be performed prior to or at the time of excision of the primary tumour.[3][7]
SLNB has been demonstrated to detect lymph node spread in up to one third of patients who would have otherwise been staged as clinically node-negative.[52]
The European Society for Medical Oncology (ESMO) MCC guideline notes that false-negative SLNBs can be seen in patients who are immunocompromised or who have tumours localised in the head, neck, or midline trunk region and/or with aberrant lymph node drainage.[19]
Result
may show metastases
Emerging tests
Merkel cell polyomavirus serology
Test
Serum testing of antibodies to Merkel cell polyomavirus (MCPyV) is available in some centres in the US. US guidelines state that it can be helpful if available, whereas European guidelines state that further prospective validation is required.[3][19] Virus-positive MCC is one of two subtypes of the disease and carries a better prognosis than UV-induced MCC.[7]
A proportion of patients with MCC caused by MCPyV develop antibodies to MCPyV oncoproteins.[53]
The baseline AMERK test is undertaken within 3 months of initial treatment.[3]
In patients who are seropositive, antibody titres can be monitored to detect changes in MCC disease burden as a rising titre may be an early indicator of recurrence.[3][53][54]
More intensive follow-up is indicated for seronegative patients as MCPyV-negative patients have a worse prognosis.[3]
Result
positive result indicates oncogenic transformation by MCPyV; post-treatment decreased oncoprotein antibody titre may indicate positive response; increasing titre may indicate disease recurrence
circulating tumour DNA (ctDNA) analysis
Test
ctDNA is a blood test that measures circulating cell-free DNA from tumour cells, thereby offering molecular disease monitoring of different cancers, including MCC. ctDNA for MCC is an emerging area of interest for disease monitoring with few published data.[55][56]
Result
may detect minimal residual MCC ctDNA
Use of this content is subject to our disclaimer