Investigations
1st investigations to order
gastroscopy
Test
Refer all patients with acute upper gastrointestinal (GI) bleeding for upper GI endoscopy (i.e., gastroscopy).[35][38][39]
If the patient is unstable with severe acute upper GI bleeding, do this urgently, immediately after resuscitation.[35][39]
For all other patients with upper GI bleeding, do this within 24 hours of admission.[35][39]
Intubate the patient before endoscopy if there is haematemesis, or there is a perceived risk of a haemodynamically unstable patient having blood in the stomach, or if the patient presents with an altered mental status (i.e., confusion).[5] Make sure the patient is appropriately resuscitated before undergoing endoscopy.
Practical tip
If the patient has been intubated, they will need to be managed in an intensive care or high-dependency unit until extubation.[5]
Gastroscopy is the gold standard technique for the diagnosis of varices and the assessment of variceal size.[5][6][7][44][45][46][47]
Variceal size is the most important predictor of haemorrhage, with the highest risk of first haemorrhage occurring in patients with large varices (15% per year).[3][4] Large varices occupy more than one third of the oesophageal lumen.[3] See the Criteria section.
The endoscopic finding of red wale marks (defined as longitudinal dilated venules resembling whip marks on the variceal surface) and the severity of liver disease are also predictive factors.[3][5][6]
[Figure caption and citation for the preceding image starts]: Large oesophageal varicesFrom the personal collection of Gennaro D'Amico, MD [Citation ends]. [Figure caption and citation for the preceding image starts]: Large oesophageal varicesFrom the personal collection of Gennaro D'Amico, MD [Citation ends].
[Figure caption and citation for the preceding image starts]: Large oesophageal varicesFrom the personal collection of Gennaro D'Amico, MD [Citation ends]. [Figure caption and citation for the preceding image starts]: (A) Grade I oesophageal varices. These collapse to inflation of the oesophagus with air. (B) Grade II oesophageal varices. These are varices between grades 1 and 3. (C) Grade III oesophageal varices. These are large enough to occlude the lumenTripathi D et al. Gut 2015;64:1680-704; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: (A) Grade I oesophageal varices. These collapse to inflation of the oesophagus with air. (B) Grade II oesophageal varices. These are varices between grades 1 and 3. (C) Grade III oesophageal varices. These are large enough to occlude the lumenTripathi D et al. Gut 2015;64:1680-704; used with permission [Citation ends].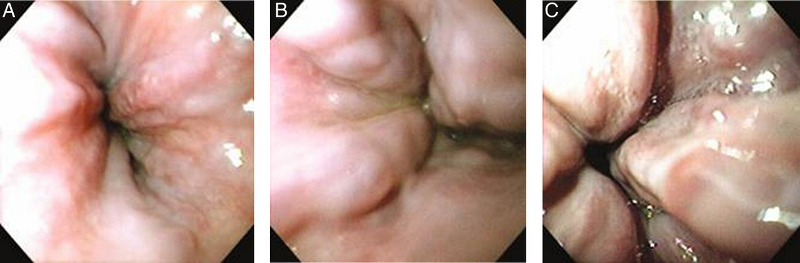
Result
dilated veins in lower oesophagus; small varices (minimally elevated veins above the oesophageal mucosa); medium varices (tortuous veins occupying less than one third of the oesophageal lumen); and large varices (occupying more than one third of the oesophageal lumen)
full blood count
Test
Patients with low mean corpuscular volume and low Hb may have variceal bleeding, or, more likely, chronic gastrointestinal occult bleeding.
Low platelet count is indicative of portal hypertension resulting from cirrhosis.
Macrocytosis is often evident in patients with chronic alcoholism.
Result
microcytic anaemia and/or thrombocytopenia
electrolytes
Test
Hyponatraemia due to volume overload or use of diuretics may be present in patients with cirrhosis with ascites.
Result
hyponatraemia
serum LFTs
Test
Measures the severity of liver disease. Aminotransferases and bilirubin may be elevated if the patient has jaundice. Albumin may be decreased if the patient is in liver failure. Total bilirubin may be normal in patients with compensated cirrhosis, but as the cirrhosis progresses, serum levels generally rise.
Result
elevated transaminases (with aspartate aminotransferase/alanine aminotransferase ratio ≥1), alkaline phosphatase, and bilirubin
serum urea and creatinine
Test
Urea can be elevated secondary to pre-renal azotaemia, acute renal insufficiency, chronic renal insufficiency, or hepatorenal syndrome in cirrhosis of the liver.
Isolated elevated serum urea (without elevated creatinine) is sometimes found as a result of breakdown of blood in the stomach in cases of acute bleeding.
Result
elevated serum urea and creatinine
coagulation profile (INR/prothrombin time)
Test
Helpful in determining the synthetic functional capacity of the liver. Elevated INR/prothrombin time indicates that patient may have cirrhosis of the liver or liver failure.
Result
normal or elevated
blood typing/cross-matching
Test
Patients with variceal haemorrhage or upper gastrointestinal bleeding from other causes can experience rapid clinical deterioration. Blood should be sent for typing and cross-matching in the event that transfusion/blood products become necessary.
Result
variable
hepatitis B surface antigen (HBsAg)
Test
May indicate hepatitis B infection as cause of cirrhosis.
Result
positive
anti-hepatitis C virus IgG (anti-HCV IgG)
Test
May indicate hepatitis C infection as cause of cirrhosis.
Result
positive
Investigations to consider
capsule endoscopy
liver ultrasound
Test
In patients with confirmed variceal bleeding, order an ultrasound to screen for portal vein thrombosis (PVT) and hepatocellular carcinoma (HCC). If ultrasound identifies PVT/HCC, seek advice on management from a gastroenterologist.
Result
PTV: filling defect in the portal vein; HCC: poorly defined margins and coarse, irregular internal echoes
Use of this content is subject to our disclaimer