Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
bracing
Many brace options are available, and the specific type of orthotic used varies from surgeon to surgeon and country to country. Braces commonly used in the US are the Boston and Rosenberger braces and the Charleston bending brace.
Several brace-wearing schedules exist, ranging from 23 hours per day to nighttime-only bracing. The International Scientific Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) consensus supports the use of an 18-hour-per-day bracing schedule.[31] Other organizations have also attempted to develop “Consensus of Care” statements and guidelines in an effort to standardize scoliosis brace treatment protocols.[31][57][58]
The goal of brace treatment is to prevent curve progression until skeletal maturity, at which time the risk of further curve progression significantly reduces.
Data from the BrAIST (Bracing in Adolescent Idiopathic Scoliosis Trial) trial have shown a significantly lower risk of curve progression in patients with AIS who wore a brace compared with those who did not.[45] One Cochrane review concluded that all of the included studies consistently showed that bracing in AIS prevented curve progression, including 7 separate studies that included a total of 662 participants.[59][Figure caption and citation for the preceding image starts]: Typical thoracic-lumbar-sacral orthosis (TLSO) scoliosis braceWeinstein SL, et al. Adolescent idiopathic scoliosis. Lancet. 2008;371:1527-1537. Used with permission [Citation ends].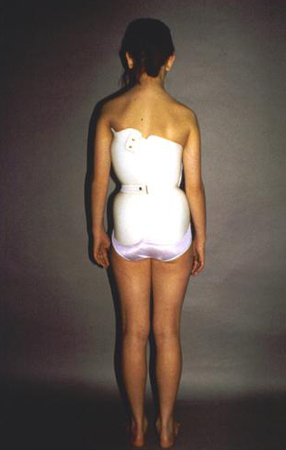
surgical spinal arthrodesis
Spinal arthrodesis with instrumentation aims to achieve maximal deformity correction, improve appearance with trunk balancing, stop continued curve progression, and reduce short- and long-term complications related to the spinal deformity.[60]
The choice of surgical approach and instrumentation technique is dictated by the characteristics of the deformity (e.g., location of the curve apex), degree of spinal flexibility, and surgeon preference.[60] Most deformities are treated with a posterior approach, although some surgeons use an anterior approach with the belief that the deformity can be corrected with a lower number of fused levels.[65][66][67][68][69][70][71][72][73] However, this approach has a higher incidence of implant failure and pseudarthrosis, and has been associated with a risk of pulmonary complications secondary to the need for "single lung" anesthesia during the procedure.[74][75][76][Figure caption and citation for the preceding image starts]: Posteroanterior scoliosis radiograph of a 13-year-old girl with a 49° right thoracic curvature with apex at the T9-T10 disc spaceFrom the collection of Stuart Weinstein, MD, University of Iowa; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Lateral scoliosis radiograph of a 13-year-old girl with a 49° right thoracic curvatureFrom the collection of Stuart Weinstein, MD, University of Iowa; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Lateral scoliosis radiograph of a 13-year-old girl with a 49° right thoracic curvatureFrom the collection of Stuart Weinstein, MD, University of Iowa; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Thirteen-year-old girl post-posterior spinal instrumentation and fusion for progressive scoliosisFrom the collection of Stuart Weinstein, MD, University of Iowa; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Thirteen-year-old girl post-posterior spinal instrumentation and fusion for progressive scoliosisFrom the collection of Stuart Weinstein, MD, University of Iowa; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Thirteen-year-old girl post-posterior spinal instrumentation and fusion for progressive scoliosisFrom the collection of Stuart Weinstein, MD, University of Iowa; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Thirteen-year-old girl post-posterior spinal instrumentation and fusion for progressive scoliosisFrom the collection of Stuart Weinstein, MD, University of Iowa; used with permission [Citation ends].
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer