Tests
1st tests to order
CBC
Test
WBC count should be <12,000 cells/mm³, because one of the four primary predictors of septic arthritis is WBC count >12,000 cells/mm³.
Result
WBC count within normal range but may be slightly elevated
erythrocyte sedimentation rate
Test
Should be <40 mm/hour, because one of the four primary predictors of septic arthritis is a rate of >40 mm/hour.
Result
within normal range but may be slightly elevated
CRP
radiograph
Test
Used primarily to rule out other disorders, such as Legg-Calvé-Perthes disease, fractures, and tumors, and for ensuring that the metaphyseal bone of the femur and acetabulum do not have signs of other processes such as osteomyelitis.[13][14][Figure caption and citation for the preceding image starts]: Radiograph of a 5-year-old child with an irritable right hip showing subtle signs early in the disease process, such as capsular distention, joint space widening, and diminution of the definition of soft-tissue planes around the hip joint or slight demineralization of the bone of the proximal femurFrom the collection of J. McCarthy [Citation ends].
Result
typically normal; however, radiographs may reveal subtle signs early in the disease process, such as capsular distention, joint space widening, diminution of the definition of soft tissue planes around the hip joint, or slight demineralization of the bone of the proximal femur
Tests to consider
ultrasound
Test
Not typically used for the diagnosis of transient synovitis, although effusions are a common finding.[15] Ultrasound can be useful for guiding needle aspiration if septic arthritis has to be excluded.[13] If septic arthritis is being considered as a differential diagnosis, joint aspiration should be performed and fluid sent for cell count and culture/Gram stain.[16][Figure caption and citation for the preceding image starts]: Ultrasound of a hip documenting a hip effusionFrom the collection of J. McCarthy [Citation ends].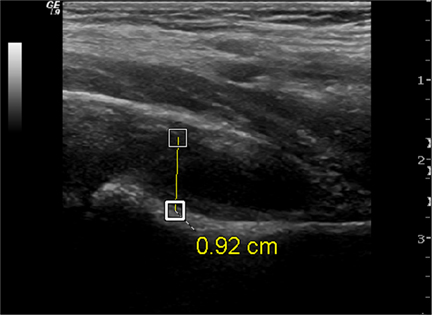
Result
increased fluid in joint
MRI with contrast
Test
Not typically used in the diagnosis of transient synovitis but rather to evaluate for other disorders, such as osteomyelitis of the proximal femur or pelvis.[13]
MRI should not be ordered for a child until all appropriate clinical, laboratory, and plain radiographic exams have been completed, unless there is concern for infection.[13][14][19]
Result
typically normal but may see fluid in the hip joint if effusion present, as noted by increased signal intensity on T2 images
Use of this content is subject to our disclaimer