Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
fluid resuscitation + contrast enema reduction
Careful monitoring is required during transit to the radiology department, as well as during the procedure. Access to monitoring and resuscitation equipment, and nursing and medical staff capable of managing a child who may become unstable, are essential.
Adequate intravenous access is required and isotonic fluid resuscitation initiated. Contrast enema (air or contrast liquid) should be performed only in patients who are clinically stable. Absolute contraindications include peritonitis, perforation, and hypovolemic shock.[28]
Reduction should be first attempted by contrast enema (air or contrast liquid) which can be both diagnostic and therapeutic.[Figure caption and citation for the preceding image starts]: Site of intussusception as revealed by abdominal x-ray, showing the meniscusFrom the collection of Dr David J. Hackam; used with permission [Citation ends].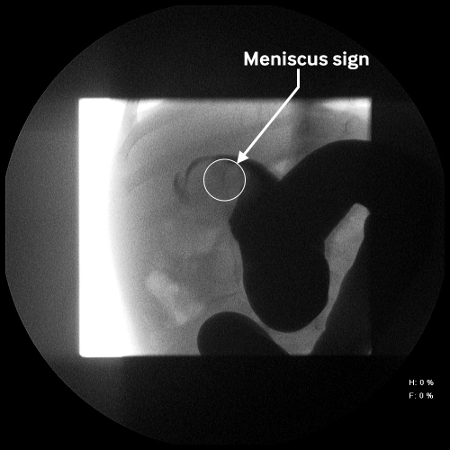 [Figure caption and citation for the preceding image starts]: Abdominal x-ray showing impaired passage of barium at site of obstruction due to intussusceptionFrom the collection of Dr David J. Hackam; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Abdominal x-ray showing impaired passage of barium at site of obstruction due to intussusceptionFrom the collection of Dr David J. Hackam; used with permission [Citation ends].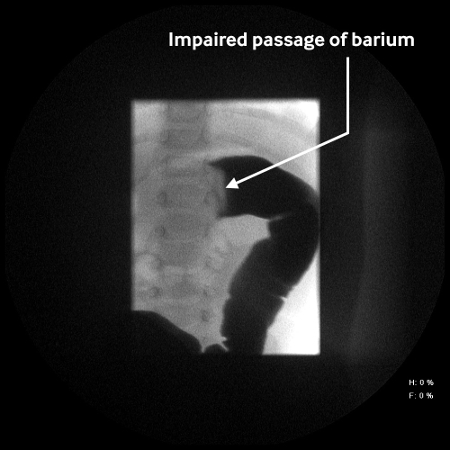 Pneumatic reduction is considered the method of choice for the treatment of intussusception in stable patients provided there is no indication for surgical reduction.[31][32] Protocols typically vary by institutions but often involve instillation of air and/or contrast at pressures ranging from 80 to 120 mm Hg.[28] The patient is kept nil by mouth.
Pneumatic reduction is considered the method of choice for the treatment of intussusception in stable patients provided there is no indication for surgical reduction.[31][32] Protocols typically vary by institutions but often involve instillation of air and/or contrast at pressures ranging from 80 to 120 mm Hg.[28] The patient is kept nil by mouth.
Barium enema: advantages over other types of contrast enema reduction include a long-standing experience in some centers, effective reduction in most cases, good evaluation for residual intussusception, and a low perforation rate. Disadvantages include the need for x-ray exposure, chemical peritonitis in the event of a perforation, and visualization of only intraluminal content. Water-soluble contrast enema has been used to reduce the risk of chemical peritonitis resulting from perforation. Reduction rate and perforation rate are comparable with other contrast agents.
Air enemas: these are noted to require less radiation and offer similar rates of failure, recurrence, and perforation to other agents.
Ultrasound-guided saline enema: excellent results have been described with the use of this modality, which offers the advantage of limiting exposure to radiation.[31][33] Although there is less experience with this method than fluoroscopic reduction, it is being used with increasing frequency in Europe and elsewhere.[21][22][32][33][34][37]
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer