Approach
Rapid resolution of symptoms occurs after treatment with vitamin C. Oral therapy is usually sufficient for most patients, although parenteral therapy may be required in some patients. The recommended daily intake varies according to numerous patient factors.
General approach to treatment
Based on current evidence, the recommended daily intake is far greater than the minimum amount needed to prevent scurvy. Should a relative deficit be identified, one should pursue the most cost-effective approach to assuring adequate nutrition, either through dietary changes to meet those needs or by daily supplementation with ascorbate preparations. Given the risk of worsening symptoms or life-threatening events, vitamin C replacement therapy should begin as soon as possible after signs and symptoms are identified. Oral replacement should be adequate for most patients. Parenteral therapy can be considered for patients with severe disease, poor enteric function or swallowing, or multiple vitamin deficiencies.[71]
Thus, best evidence suggests at least 300-500 mg/day of vitamin C (ascorbic acid) for adults. The optimum dose for children is not determined, but should be at least the recommended daily intake. The maximum daily doses for subgroups are outlined in the accompanying table of recommended daily intake to prevent vitamin C deficiency, and are based on actual and theoretical adverse risks as identified in experimental models and human trials of megadose vitamin C for various conditions. After at least 2 weeks of vitamin C replacement therapy, the general approach to prevention of vitamin C deficiency should be assumed. Chronic supplementation with vitamin C may be indicated in some people.
The recommended daily intake of vitamin C varies by age, sex, pregnancy, lactation, and smoking status.[Figure caption and citation for the preceding image starts]: Recommended daily quantity of vitamin C to prevent deficiency. The appropriate RDA has been disputed in several large reviews. These guidelines are drawn from the most recent published large consensus of appropriate intake based on data from historical, biologic, epidemiologic, and intervention studiesFrom: Panel on Dietary Antioxidants and Related Compounds, Subcommittees on Upper Reference Levels of Nutrients and Interpretation and Uses of DRIs, Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Food and Nutrition Board, Institute of Medicine. Chapter 5: vitamin C. In: Food and Nutrition Board, Institute of Medicine's Dietary reference intakes for vitamin C, vitamin E, selenium, and carotenoids. Washington DC: National Academy Press; 2000: 95-185 [Citation ends].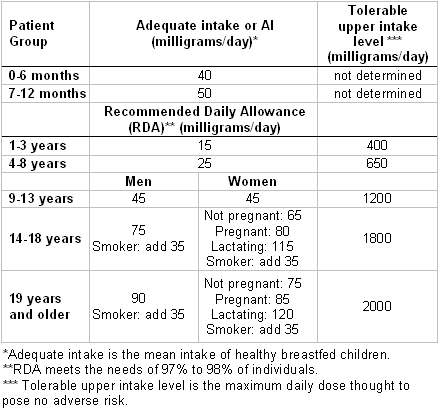
For hospitalized and critically sick patients, no apparent consensus exists in the medical literature for the exact amount of vitamin C supplementation to prevent and treat vitamin C deficiency. However, European Society for Clinical Nutrition and Metabolism recommends the following:[62]
Daily recommended dose for adults receiving parenteral nutrition is 100-200 mg/day
Daily recommended dose for adults with chronic oxidative stress is 200-500 mg/day
Daily recommended dose for adults during critical illness or continuous renal replacement therapy is 2-3 g/day (given intravenously).
However, recent studies have shown that adjunctive vitamin C therapy has not been shown to improve outcomes and may even worsen outcomes in patients with acute respiratory distress syndrome or sepsis, respectively.[51][72] Therefore, supplementation of vitamin C is not recommended beyond the recommended daily intake in the setting of critical illness.
Presumptive treatment
There is no apparent contraindication to normal doses of vitamin C as empiric therapy. In all contexts, but particularly in medical facilities with limited resources, empiric treatment may provide a diagnosis if supportive resources are not immediately available. In patients with scurvy, the improvement in signs and symptoms is often rapid, initially within days once body stores achieve a level sufficient to meet the needs of vitamin C-dependent pathways (typically above 300 mg total body store), and may yield diagnostic information in a similar time frame.
Use of this content is subject to our disclaimer