Tests
Tests to consider
skin biopsy
Test
The underlying dermis demonstrates superficial fibroplasia and a variable inflammatory infiltrate depending on the presence or absence of an underlying inflammatory dermatosis. [Figure caption and citation for the preceding image starts]: Low-power photomicrograph of lichen simplex chronicus (hematoxylin-eosin stain, x40)From the personal collection of Dr Brian L. Swick; used with permission [Citation ends].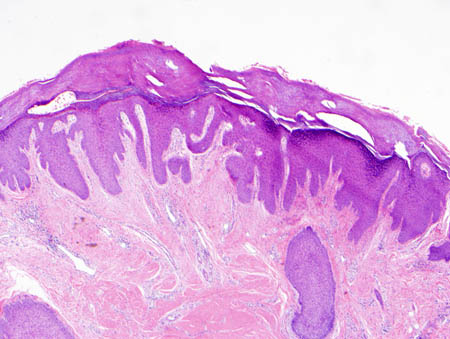 [Figure caption and citation for the preceding image starts]: Medium-power photomicrograph of lichen simplex chronicus (hematoxylin-eosin stain, x100)From the personal collection of Dr Brian L. Swick; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Medium-power photomicrograph of lichen simplex chronicus (hematoxylin-eosin stain, x100)From the personal collection of Dr Brian L. Swick; used with permission [Citation ends].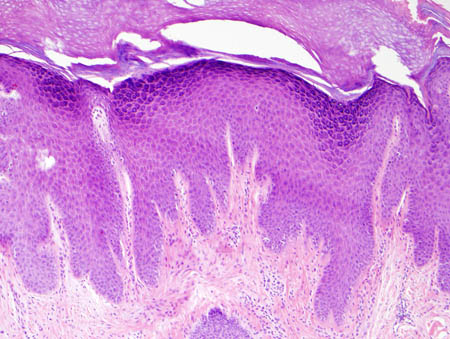 [Figure caption and citation for the preceding image starts]: High-power photomicrograph of lichen simplex chronicus (hematoxylin-eosin stain, x200)From the personal collection of Dr Brian L. Swick; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: High-power photomicrograph of lichen simplex chronicus (hematoxylin-eosin stain, x200)From the personal collection of Dr Brian L. Swick; used with permission [Citation ends].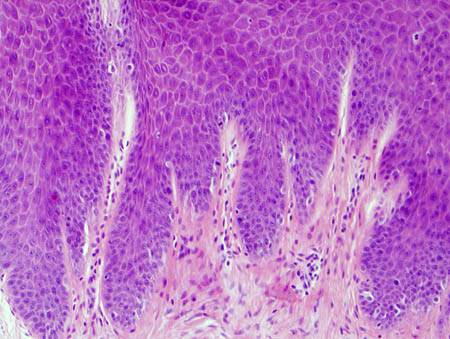
Only required if the history and physical exam findings are atypical or to exclude other similar-appearing dermatoses such as hypertrophic lichen planus, multiple keratoacanthomata, and pemphigoid nodularis.[1][22]
It may also be useful to detect an underlying pruritic inflammatory dermatosis driving secondary LSC.
It may also be indicated for lesions that do not show appropriate response to therapy, to confirm the original diagnosis and exclude a cutaneous malignancy such as squamous cell carcinoma.
Result
irregular psoriasiform epidermal hyperplasia with hyperkeratosis, focal parakeratosis, and often hypergranulosis
patch testing
Test
Only required if secondary LSC due to a contact allergen is suspected. In addition, it may be helpful in excluding allergic contact dermatitis to topical corticosteroids used in the treatment of LSC. This is especially pertinent if the condition paradoxically worsens during such treatment.
The only FDA-approved patch test panel available is the TRUE (thin-layer rapid-use epicutaneous) test, which tests 24 common contact allergens.[23]
A positive test with the TRUE test panel does not confirm that the antigen in question is responsible for the eruption. One study found that 62% of patients had at least 1 positive reaction on the TRUE test, of which only 45% were relevant to the current eruption.[24]
Result
positive dermatitic reaction to a relevant antigen
potassium hydroxide preparation
Test
Undertaken in the doctor's office. Scale from a skin lesion is placed on a glass slide, treated with potassium hydroxide solution to dissolve the scale, and viewed under a microscope.
Only required if secondary LSC due to an underlying dermatophyte or Candida infection is suspected. One study found the sensitivity and specificity of this test, when undertaken by general practice physicians, to be 12% and 93%, respectively.[25]
Result
septate hyphae in dermatophyte infection, pseudohyphae with budding yeast in Candida infection
fungal culture
Test
Clinically relevant fungi are those that are known to cause the condition and are not commensals or contaminants.
Culture of scale from a skin lesion. Consider a vaginal fungal culture for underlying vulvovaginal candidiasis in patients with vulvar LSC.[22]
Only required if secondary LSC due to an underlying dermatophyte or Candida infection is suspected. Results may be falsely negative secondary to inadequate sample size, a specimen poor in fungal elements, suboptimal culture conditions (insufficient incubation time, unsuitable temperature, presence of contaminants), and use of antifungal agents before sampling.[26]
Result
growth of clinically relevant fungi
skin scrapings
Test
Undertaken in the doctor's office. Scrapings taken from a suspected scabies burrow are placed on a glass slide and viewed under a microscope.[27]
Only required if secondary LSC due to scabies infestation is suspected. The sensitivity of this test is only 50% due to the low numbers of the parasite present in an immunocompetent host.[28]
Result
presence of mites, eggs, or scybala
serum TSH and free T4
Test
Only required if secondary LSC due to hypo- or hyperthyroidism is suspected.
Result
TSH elevated with low free T4 in hypothyroidism, TSH low with elevated free T4 in hyperthyroidism
serum creatinine and BUN and electrolytes
Test
Only required if secondary LSC due to renal failure is suspected.
Result
creatinine elevated, BUN elevated, and hyperkalemia in renal failure
LFTs and gamma-GT
Test
Only required if secondary LSC due to cholestasis is suspected. Obstructive biliary disease (primary biliary cirrhosis and primary sclerosing cholangitis) shows characteristic derangement of LFTs and gamma-GT.
Result
AST and ALT minimally abnormal, alkaline phosphatase elevated, gamma-GT elevated in cholestasis
CBC
Test
Only required if secondary LSC due to polycythemia rubra vera is suspected.
Result
hematocrit >60% in males, >55% in females in polycythemia rubra vera
Use of this content is subject to our disclaimer