History and exam
Key diagnostic factors
common
fatigue and effort intolerance
dyspnea
palpitations
Related to atrial arrhythmia (flutter, fibrillation).
jugular venous abnormality
The abnormal and prominent v wave in the jugular venous pulse indicates the pressure wave of right ventricle systole transmitted through the incompetent tricuspid valve.[7]
irregular heart rhythm
Sign of atrial flutter or fibrillation.
parasternal systolic murmur
Lower left parasternal systolic murmur (holosystolic or less than holosystolic, depending on severity of hemodynamic derangement).[7]
increased systolic murmur on inspiration (Carvallo sign)
Increased systolic murmur on inspiration.[7]
Other diagnostic factors
uncommon
abdominal distension
early satiety, dyspepsia, or indigestion
liver and systemic venous pulsation
An enlarged and pulsatile liver is usually seen in severe TR, and is caused by reverse blood flow to the liver during systole. Severe TR can even result in systemic venous pulsation, for example with pulsatile varicose veins.[17]
Risk factors
strong
left-sided heart failure
The most common cause of right heart failure. Most clinically significant TR occurs from elevation of right ventricular systolic and/or diastolic pressure, right ventricular cavity enlargement, or tricuspid annular dilation secondary to left-sided cardiac pathology in the form of advanced mitral, aortic, and left ventricular myocardial disorders.[1][5]
dilated tricuspid annulus
The tricuspid valve orifice area is decreased during atrial and ventricular systole, supporting the concept that "contraction" of the tricuspid valve annulus contributes to normal closure of the valve. Any abnormality that impairs function of the annulus can result in valve regurgitation. Tricuspid valve annulus dilation is most commonly secondary to chronic heart failure, left-sided rheumatic valvular heart disease, or less often, pulmonary hypertension.[8][Figure caption and citation for the preceding image starts]: Severe tricuspid regurgitation due to annular enlargement. A. Systolic frame from apical 4 chamber view (Mayo Clinic display format with right ventricle on the right). Note tricuspid annular enlargement measuring 4.2 cm and tethering of the tricuspid leaflets leading to failure of coaptation of the tricuspid valve. B. Massive tricuspid regurgitation on Color Doppler. C. Continuous Wave Doppler through the tricuspid valve. Note the dagger-shaped tricuspid regurgitant signal (arrows), consistent with rapid equalization of pressures between right ventricle and right atrium, typical of massive tricuspid regurgitation. D. Pulsed Wave Doppler of the hepatic veins demonstrates late systolic flow reversals consistent with severe tricuspid regurgitation.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends].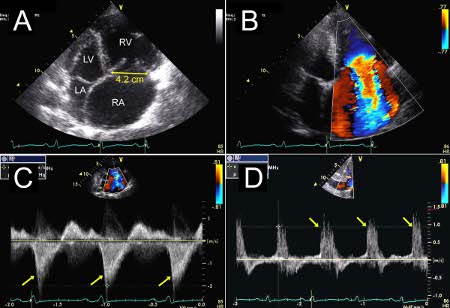
rheumatic heart disease
endocarditis
Acquired cause of TR.
carcinoid heart disease
Acquired cause of TR that can cause scarring of the valve.[Figure caption and citation for the preceding image starts]: Severe tricuspid regurgitation due to carcinoid valvular disease. A. Systolic frame from mid-esophageal 4 chamber view. Note thickened tricuspid leaflets, but also retracted and thickened chordae, typical of advanced carcinoid valvular disease (arrows). The right ventricle and right atrium are enlarged. The atrial septum is deviated to the left, demonstrating right atrial pressure is higher than left atrial pressure (asterisk). B. Color Doppler demonstrating severe tricuspid regurgitation. Vena contracta measured 1.2 cm, consistent with the coaptation gap on 2D images and virtually free flow between the right ventricle and right atrium.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends].
weak
pacemaker lead entrapment
Insertion of a pacemaker or an internal cardiac defibrillator lead regularly results in mild regurgitation. However, damage to the tricuspid valve or leaflet restriction by the lead may produce moderate or severe symptomatic TR and may not be overtly visualized by echocardiography.[12][Figure caption and citation for the preceding image starts]: Tricuspid valve entrapped with a pacemaker leadFrom the collection of Dr Thoraf M. Sundt III [Citation ends].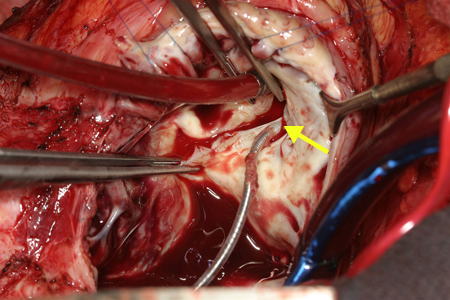 [Figure caption and citation for the preceding image starts]: Two patients referred for severe tricuspid regurgitation after pacemaker implantation. A, C. Apical 4 chamber views (Mayo Clinic display format with right ventricle on the right) showing impingement of tricuspid leaflets by pacemaker leads (arrows). Note presence of two right ventricular leads in the first patient (panel A; one active, one abandoned lead). B, D. Corresponding Color Doppler images demonstrating severe tricuspid regurgitation due to lead impingement.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends].
[Figure caption and citation for the preceding image starts]: Two patients referred for severe tricuspid regurgitation after pacemaker implantation. A, C. Apical 4 chamber views (Mayo Clinic display format with right ventricle on the right) showing impingement of tricuspid leaflets by pacemaker leads (arrows). Note presence of two right ventricular leads in the first patient (panel A; one active, one abandoned lead). B, D. Corresponding Color Doppler images demonstrating severe tricuspid regurgitation due to lead impingement.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends].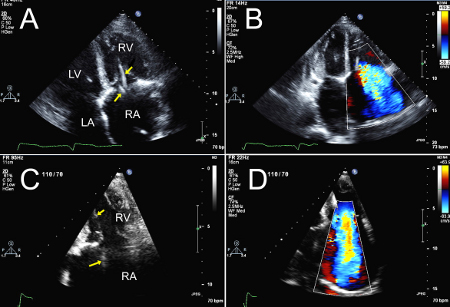
ischemic cardiomyopathy
constrictive pericarditis
Risk factor for left-sided heart failure and subsequent TR.[1]
toxins
Risk factor for TR such as phentermine-fenfluramine (Phen-Fen) valvulopathy or methysergide valvulopathy.[1]
rheumatoid arthritis
Less common acquired cause.
radiation therapy
Less common acquired cause.
trauma
For example, repeated endomyocardial biopsies or severe blunt chest trauma injury.
Marfan syndrome
Less common acquired cause.
tricuspid valve prolapse
Less common acquired cause.
Use of this content is subject to our disclaimer