Etiology
TR occurs with abnormal (primary) or normal (secondary, functional) valve morphology. Causes of primary valve dysfunction are uncommon, and include congenital etiologies such as cleft valve in association with atrioventricular canal defect and Ebstein anomaly; acquired etiologies include rheumatic valvulitis, endocarditis, or scarring from carcinoid heart disease.[6] Less commonly, TR occurs with rheumatoid arthritis, Marfan syndrome, pacemaker lead entrapment, and tricuspid valve prolapse (sometimes in association with myxomatous mitral valve disease), or following trauma (such as blunt force trauma or repeated endomyocardial biopsies), radiation therapy, and toxin exposure (phentermine-fenfluramine [Phen-Fen] or methysergide). The most clinically significant form of TR, however, is secondary in nature, commonly due to left-sided cardiac pathology in the form of advanced mitral, aortic, and left ventricular myocardial disorders.[1][5][6][Figure caption and citation for the preceding image starts]: Severe tricuspid regurgitation due to carcinoid valvular disease. A. Systolic frame from mid-esophageal 4 chamber view. Note thickened tricuspid leaflets, but also retracted and thickened chordae, typical of advanced carcinoid valvular disease (arrows). The right ventricle and right atrium are enlarged. The atrial septum is deviated to the left, demonstrating right atrial pressure is higher than left atrial pressure (asterisk). B. Color Doppler demonstrating severe tricuspid regurgitation. Vena contracta measured 1.2 cm, consistent with the coaptation gap on 2D images and virtually free flow between the right ventricle and right atrium.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends]. [Figure caption and citation for the preceding image starts]: Tricuspid valve entrapped with a pacemaker leadFrom the collection of Dr Thoraf M. Sundt III [Citation ends].
[Figure caption and citation for the preceding image starts]: Tricuspid valve entrapped with a pacemaker leadFrom the collection of Dr Thoraf M. Sundt III [Citation ends].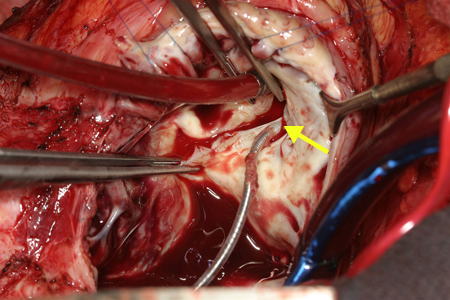 [Figure caption and citation for the preceding image starts]: Two patients referred for severe tricuspid regurgitation after pacemaker implantation. A, C. Apical 4 chamber views (Mayo Clinic display format with right ventricle on the right) showing impingement of tricuspid leaflets by pacemaker leads (arrows). Note presence of two right ventricular leads in the first patient (panel A; one active, one abandoned lead). B, D. Corresponding Color Doppler images demonstrating severe tricuspid regurgitation due to lead impingement.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends].
[Figure caption and citation for the preceding image starts]: Two patients referred for severe tricuspid regurgitation after pacemaker implantation. A, C. Apical 4 chamber views (Mayo Clinic display format with right ventricle on the right) showing impingement of tricuspid leaflets by pacemaker leads (arrows). Note presence of two right ventricular leads in the first patient (panel A; one active, one abandoned lead). B, D. Corresponding Color Doppler images demonstrating severe tricuspid regurgitation due to lead impingement.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends].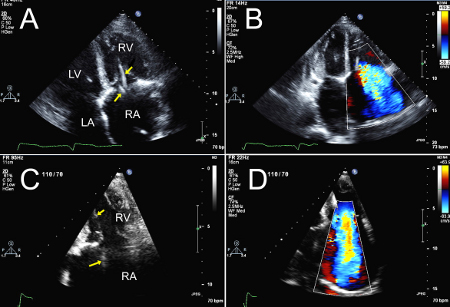
Pathophysiology
Normal tricuspid valves develop dysfunction with elevation of right ventricular systolic and/or diastolic pressure, right ventricular cavity enlargement, or tricuspid annular dilation with leaflet tethering.[1][5][6] The pathologic consequences of advanced TR are related to a reduced cardiac output and elevated right atrial pressure, which, if longstanding, leads to atrial distension with reduced contractile reserve and atrial fibrillation.[7] Often, patients with chronic severe TR will present with ascites from advanced liver disease from chronic congestion or fibrosis (cardiac cirrhosis), gut congestion with symptoms of dyspepsia or indigestion, and fluid retention with leg edema.[6][Figure caption and citation for the preceding image starts]: Severe tricuspid regurgitation due to annular enlargement. A. Systolic frame from apical 4 chamber view (Mayo Clinic display format with right ventricle on the right). Note tricuspid annular enlargement measuring 4.2 cm and tethering of the tricuspid leaflets leading to failure of coaptation of the tricuspid valve. B. Massive tricuspid regurgitation on Color Doppler. C. Continuous Wave Doppler through the tricuspid valve. Note the dagger-shaped tricuspid regurgitant signal (arrows), consistent with rapid equalization of pressures between right ventricle and right atrium, typical of massive tricuspid regurgitation. D. Pulsed Wave Doppler of the hepatic veins demonstrates late systolic flow reversals consistent with severe tricuspid regurgitation.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends].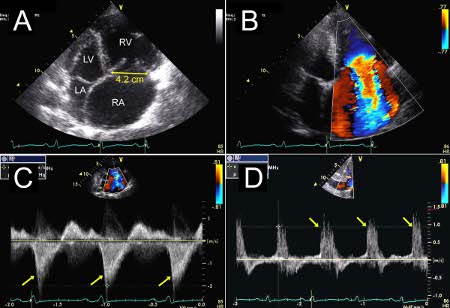
Classification
TR severity as determined by echocardiographic quantification of annular diameter
Normal tricuspid valve annulus diameter in adults is 28 mm (± 5 mm) in the 4 chamber view. Significant tricuspid annular dilation is defined by a diastolic diameter of over 40 mm (absolute value) or 21 mm/square meter of body surface area.[2] A correlation exists between tricuspid annulus diameter and TR severity: a systolic tricuspid diameter >3.2 cm or a diastolic tricuspid annulus diameter >3.4 cm are often markers of more significant TR.[3][Figure caption and citation for the preceding image starts]: Severe tricuspid regurgitation due to annular enlargement. A. Systolic frame from apical 4 chamber view (Mayo Clinic display format with right ventricle on the right). Note tricuspid annular enlargement measuring 4.2 cm and tethering of the tricuspid leaflets leading to failure of coaptation of the tricuspid valve. B. Massive tricuspid regurgitation on Color Doppler. C. Continuous Wave Doppler through the tricuspid valve. Note the dagger-shaped tricuspid regurgitant signal (arrows), consistent with rapid equalization of pressures between right ventricle and right atrium, typical of massive tricuspid regurgitation. D. Pulsed Wave Doppler of the hepatic veins demonstrates late systolic flow reversals consistent with severe tricuspid regurgitation.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends].
Vena contracta width quantification of TR
Severe TR is defined as vena contracta (the narrowest central flow region of a jet that occurs at, or just downstream to, the orifice of a regurgitant valve) width >0.7 cm.[Figure caption and citation for the preceding image starts]: Severe tricuspid regurgitation due to carcinoid valvular disease. A. Systolic frame from mid-esophageal 4 chamber view. Note thickened tricuspid leaflets, but also retracted and thickened chordae, typical of advanced carcinoid valvular disease (arrows). The right ventricle and right atrium are enlarged. The atrial septum is deviated to the left, demonstrating right atrial pressure is higher than left atrial pressure (asterisk). B. Color Doppler demonstrating severe tricuspid regurgitation. Vena contracta measured 1.2 cm, consistent with the coaptation gap on 2D images and virtually free flow between the right ventricle and right atrium.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends]. In case of multiple jets, the respective values of the vena contracta width are not additive.[3]
Echocardiography Doppler quantification of TR
Proximal isovelocity surface area (PISA) radius of 1 mm to 4 mm suggests mild TR, 5 mm to 8 mm moderate TR, and >9 mm severe TR, at an aliasing velocity setting (the velocity of a flow that exceeds the color Doppler scale) of approximately 40 cm/second. An effective regurgitant orifice area ≥40 mm² or a regurgitant volume of ≥45 mL indicates severe TR. The PISA method may underestimate the severity of TR; it is less accurate in multiple jets.[3] Quantification is important, as there is great variability in interpreting TR severity based on semi-quantitative indices alone.[4]
Doppler color flow jet quantification of TR
The color flow area of the regurgitant jet is not recommended to quantify the severity of TR.[Figure caption and citation for the preceding image starts]: Severe tricuspid regurgitation due to annular enlargement. A. Systolic frame from apical 4 chamber view (Mayo Clinic display format with right ventricle on the right). Note tricuspid annular enlargement measuring 4.2 cm and tethering of the tricuspid leaflets leading to failure of coaptation of the tricuspid valve. B. Massive tricuspid regurgitation on Color Doppler. C. Continuous Wave Doppler through the tricuspid valve. Note the dagger-shaped tricuspid regurgitant signal (arrows), consistent with rapid equalization of pressures between right ventricle and right atrium, typical of massive tricuspid regurgitation. D. Pulsed Wave Doppler of the hepatic veins demonstrates late systolic flow reversals consistent with severe tricuspid regurgitation.From the collection of Sorin V. Pislaru, Mayo Clinic [Citation ends]. Color flow imaging should only be used for diagnosing TR. A more quantitative approach is required when more than a small central TR jet is observed.[3]
Inferior vena cava flow reversal quantification of TR
The systolic hepatic flow reversal is specific for severe TR. It represents the strongest additional parameter for evaluating the severity of TR.[3] Concomitant presence of atrial fibrillation or right ventricular pacing reduces the specificity of this finding.
Use of this content is subject to our disclaimer