History and exam
Key diagnostic factors
common
exertional dyspnea
One of the most common presenting symptoms, alongside fatigue.
Dyspnea occurs at a prevalence of 60%.[27]
fatigue
One of the most common presenting symptoms together with exertional dyspnea.
chest pain
Patients frequently develop exertional chest pain (angina). Symptoms may occur even in the absence of coronary atherosclerotic disease.
Chest pain occurs at a prevalence of 50%.[27]
exertional syncope
A classic symptom and may be caused by arrhythmia or postural hypotension related to AS.
The prevalence of syncope is 40%.[27]
ejection systolic murmur
A systolic murmur ≥3/6 is present with a crescendo-decrescendo pattern that peaks in midsystole and radiates to the carotid. The peak moves later in systole as the AS becomes more severe.
The murmur is loudest at the right upper sternal border.[Figure caption and citation for the preceding image starts]: The systolic crescendo-decrescendo murmur of aortic stenosisFrom the collection of David Liff, MD, Emory University Hospital; used with permission [Citation ends].
S2 diminished and single
With progression of AS, the aortic component of the second heart sound becomes soft or absent due to decreased mobility of the aortic valve leaflets.
Aortic valve closure is delayed and often coincides with pulmonic valve closure, producing a single second heart sound.
uncommon
carotid parvus et tardus
The carotid upstroke is frequently delayed and diminished in severe AS (parvus et tardus).
This finding is often absent in older patients with less compliant vasculature. In these circumstances, palpation of the brachial artery may reveal this finding.
Other diagnostic factors
uncommon
paradoxically split S2
With more severe stenosis, aortic valve closure may become so delayed that it follows pulmonic valve closure during expiration, producing the paradoxically split S2.
May be accentuated by left bundle branch block.
Gallavardin phenomenon
A musical-quality, holosystolic murmur is present at the apex of the heart that occurs in older patients with calcific AS, which may mimic mitral regurgitation.
bleeding
Some patients may develop an acquired von Willebrand deficiency that predisposes to bleeding and is caused by turbulent flow across the stenotic valve.[41] Patients may describe epistaxis or bruising. They are also more likely to develop chronic gastrointestinal bleeding that is associated with angiodysplasia.[41]
Risk factors
strong
age >60 years
AS typically presents in the seventh or eighth decade for patients with trileaflet valves and two decades earlier for patients with bicuspid valves.[6]
Although the prevalence of AS is only 0.2% in adults ages 50 to 59 years, estimates increase to 1.3% in patients ages 60 to 69 years, and up to 9.8% in patients ages 80 to 89 years.[14] Overall, AS is present in 2.6% of adults older than 75 years of age.[10]
congenitally bicuspid aortic valve
Present in the majority of patients younger than 70 years of age who undergo valve replacement for severe aortic stenosis.[15]
Unicuspid and bicuspid valves experience abnormal shear and mechanical stresses from birth. Therefore, the pathologic processes and resultant stenosis occur earlier than in trileaflet valves.[6][7][13][Figure caption and citation for the preceding image starts]: Bicuspid and trileaflet aortic valves with severe calcification following surgical excisionFrom the collection of David Liff, MD, Emory University Hospital; used with permission [Citation ends].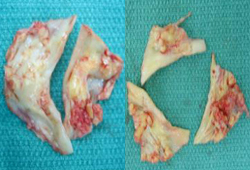
rheumatic heart disease
Common cause of AS in developing countries.
In rheumatic disease, an autoimmune inflammatory reaction is triggered by prior Streptococcus infection that targets the valvular endothelium, leading to inflammation and eventually calcification.
chronic kidney disease
AS is prevalent in people with chronic kidney disease; progression of AS in these patients is typically rapid and unpredictable.[12] Aortic valve calcification occurs in up to 55% of dialysis patients ages >65 years.[16] Dialysis patients also have more rapid annual decrease in valve area (0.23 cm² vs. 0.1 cm²) compared with patients with normal renal function.[12][16]
weak
radiation therapy
AS is a rare complication of mediastinal radiation therapy that presents at least 2 decades following treatment.[17]
high low-density lipoprotein (LDL) cholesterol
Retrospective studies have demonstrated that high LDL-cholesterol levels are associated with AS, and several small studies have found that statin therapy targeting LDL-cholesterol slows the hemodynamic progression of AS.[18] However, these findings were not verified in a large prospective study.[19] Dyslipidemia is significantly associated with an increased risk of developing severe AS.[3][20]
hyperlipoproteinemia
Familial hypercholesterolemia is a rare genetic disorder that can contribute to early-onset calcification of the aortic valve and the aortic root.[21]
hypertension
elevated lipoprotein(a)
Elevated lipoprotein(a) is associated with an increased risk of cardiovascular disease and aortic stenosis.[9]
family history
Use of this content is subject to our disclaimer