Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
surgery
Surgical treatment is rarely performed, and is only indicated in patients with extensive symptoms who fail conservative and percutaneous treatment.
It is the experience of some surgeons that simple excision of a popliteal cyst results in high incidence of recurrence.
Surgical options have been described, including anterior open synovectomy, arthroscopic synovectomy, radiosynovectomy, capsulectomy, capsuloplasty with pedicle graft, and repair of joint capsule.
Arthroscopic resection facilitates management of the cyst, by arthroscopic decompression, and the associated intra-articular disorder. Surgery involves enlarging the interval between the semimembranosus and medial gastrocnemius, allowing the cyst contents to drain into the joint.
Arthroscopic resection is effective, and is associated with reduced morbidity and recurrence compared with excision.[24][25][26][Figure caption and citation for the preceding image starts]: Arthroscopic resection of a popliteal cystFrom the collection of Dr John Kelly IV; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Arthroscopic resection of a popliteal cystFrom the collection of Dr John D. Kelly IV; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Arthroscopic resection of a popliteal cystFrom the collection of Dr John D. Kelly IV; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Septae within a popliteal cystFrom the collection of Dr John D. Kelly IV; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Septae within a popliteal cystFrom the collection of Dr John D. Kelly IV; used with permission [Citation ends].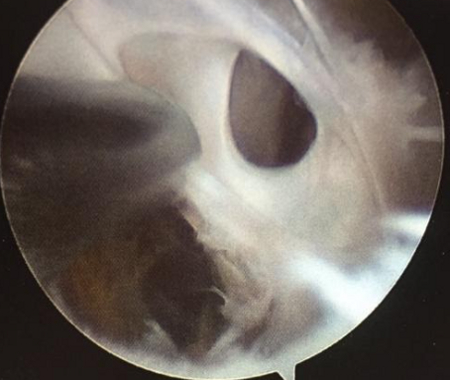
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer