History and exam
Key diagnostic factors
common
popliteal bulge
Popliteal cysts are usually visible as a bulge behind the knee, particularly noticeable upon standing and in comparison to the opposite uninvolved knee.
They are generally soft and minimally tender.
It is common for a popliteal cyst to expand and shrink over time.
knee pain
Patients may present with knee pain from the cyst itself or the underlying cause of the cyst, such as arthritis, an injury, or a mechanical problem with the knee such as a meniscal tear.
leg swelling
Popliteal cyst dissection and rupture are frequently associated with swelling of the leg mimicking deep vein thrombosis.
calf tenderness
Patients with a large cyst, especially one that may have ruptured, will have tenderness in the calf during examination.
Other diagnostic factors
uncommon
calf ecchymosis
Rupture of a popliteal cyst may lead to: leaking of fluid down the inner leg, sometimes causing the inner ankle to have the appearance of a painless bruise; calf ecchymosis, with significant pain; and, rarely, compartment syndrome, presenting with sensory or motor deficits secondary to elevated intracompartmental pressures.
Risk factors
strong
knee joint trauma
Injury of the medial meniscus, chondral lesions, and tears of the anterior cruciate ligament are well-described significant risk factors in development of popliteal cysts.
Results in overproduction of synovial fluid and increased intra-articular pressure that leads the synovial capsule to bulge at an area where there is a lack of external anatomic support.[1][Figure caption and citation for the preceding image starts]: Popliteal cyst lying in its most common location in the posteromedial popliteal fossa (A), dissecting through the deep fascia (B) and the medial head of the gastrocnemius muscle (C)Adapted from Labropoulos N, Shifrin DA, Paxinos O. New insights into the development of popliteal cysts. Br J Surg. 2004;91:1313-1318; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Deep dissection of the posteromedial capsule. The 2 expansions of the semimembranosus muscle have been elevated, exposing the weak area of the capsule between the posterior cruciate ligament (A) and the posterior horn of the medial meniscus (B) that gives entry to the knee joint. The medial femoral condyle is also visible (C)Adapted from Labropoulos N, Shifrin DA, Paxinos O. New insights into the development of popliteal cysts. Br J Surg. 2004;91:1313-1318; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Deep dissection of the posteromedial capsule. The 2 expansions of the semimembranosus muscle have been elevated, exposing the weak area of the capsule between the posterior cruciate ligament (A) and the posterior horn of the medial meniscus (B) that gives entry to the knee joint. The medial femoral condyle is also visible (C)Adapted from Labropoulos N, Shifrin DA, Paxinos O. New insights into the development of popliteal cysts. Br J Surg. 2004;91:1313-1318; used with permission [Citation ends].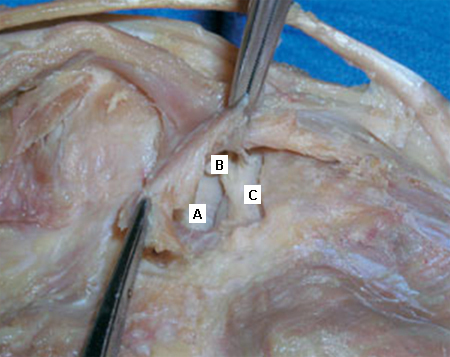
underlying knee joint arthritis or synovitis
Results in overproduction of synovial fluid, which leads to increased pressure and bulging of the synovial capsule.[1] Pigmented villonodular synovitis should also be suspected.[16]
Patients with a history of joint pathology (arthritis or joint trauma) have a 15% to 40% prevalence of popliteal cysts.[5][6][7]
underlying knee joint infection
increasing age
Prevalence of cysts increases with age: 26% in patients ages 31 to 50 years, and 53% in patients ages 51 to 90 years.[9]
Use of this content is subject to our disclaimer