Investigations
1st investigations to order
FBC
renal function
liver function tests
Test
May identify cholestasis secondary to hepatic metastasis.[48]
Baseline values prior to start of potentially hepatotoxic chemotherapy are useful.
Result
normal or elevated aspartate aminotransferase, alanine aminotransferase, and serum bilirubin
urinalysis
Test
Visible or non-visible haematuria may be a presenting sign.[3]
Proteinuria may be found in patients with Denys-Drash syndrome.
Result
clear/red colour, red blood cell >3/high power field, protein >30 mg/dL or normal
serum total protein/albumin
Test
Cachexia and poor oral intake may lead to lower serum albumin/total protein.
Rarely, proteinuria may result in hypoalbuminaemia in patients with bilateral Wilms' tumour or Denys-Drash syndrome.[49]
Result
normal or low
coagulation studies
serum calcium level
Test
May be due to bone metastasis and elevated PTH from a more aggressive renal tumour.[51]
Result
normal or elevated
abdominal ultrasound with Doppler
Test
Initial test of choice for presumptive diagnosis.
Relatively easy to perform without sedation in young children and establishes the renal origin of the mass, assesses the full number and location of renal masses, and uses duplex ultrasound scan to determine the presence of a tumour thrombus in the renal vein and inferior vena cava.[38]
Result
evenly echogenic, heterogenous, mainly solid mass arising from kidney(s) with or without cystic areas
CT or MRI abdomen and pelvis with and without contrast
Test
Confirms ultrasound findings and defines extent of the tumour for staging.[38][Figure caption and citation for the preceding image starts]: Wilms' tumour: MRI findingsUHRAD.com; used with permission [Citation ends].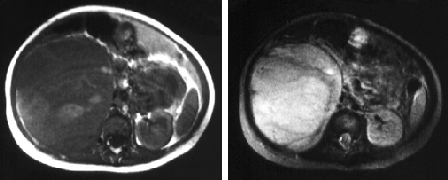
This includes evaluating the contralateral kidney for synchronous disease; determining the size and number of ipsilateral masses; assessing for the presence of lymphadenopathy, signs of possible rupture, and infiltration into adjacent organs; the presence and extent of tumour thrombus; and the presence of metastatic disease to organs such as the liver.[38]
Children's Oncology Group (COG) protocols support the use of CT or MRI for locoregional staging; the International Society of Paediatric Oncology - Renal Tumour Study Group (SIOP-RTSG) prefers MRI over CT for abdominopelvic evaluation.[38]
MRI is strongly recommended over CT in case of bilateral or genetically predisposed Wilms' tumours, as it may help identify multifocal tumours and nephrogenic rests.[38][52][53]
Enough for a presumptive diagnosis, but review of histology is necessary for a definitive diagnosis.
Result
renal mass with heterogeneous enhancement; extrarenal lesions associated with metastatic disease
CT chest with and without contrast
Test
Lungs are the most frequently occurring site of metastases for Wilms' tumour; however, differentiation of malignant and benign pulmonary nodules remains challenging.[38] The International Society of Paediatric Oncology (SIOP) protocol classifies pulmonary nodules ≥3 mm as lung metastases, but there is significant observer variability such that use of this threshold is questioned.[54]
Result
pulmonary lesions associated with metastatic disease
chest x-ray
Test
In resource-limited regions, chest x-ray can be used to identify lung metastasis; however, plain radiography may miss smaller pulmonary lesions (typically <1 cm).[3]
Chest x-ray may be used for disease surveillance at follow-up.[38]
Result
pulmonary lesions; hilar and/or mediastinal widening due to lymphadenopathy may be identified
Investigations to consider
tumour histology
Test
Definitive diagnosis is based on histology of tumour following surgical resection (nephrectomy) or biopsy (if tumour is unresectable).[3]
An open biopsy with a minimum of 10-12 cores is required in the Children's Oncology Group (COG) protocol if a tumour is unresectable.[3] In the International Society of Paediatric Oncology (SIOP) UMBRELLA protocol, pretreatment biopsy is not routinely recommended.[41] Percutaneous cutting needle biopsy (tru-cut biopsy) can be considered in patients whose tumours are suspected not to be Wilms' tumour, such as young children with stage IV disease and in children >10 years of age, as the frequency of non-Wilms renal tumours is increased in these age groups.[41][42]
All three lineages of the developing kidney (blastema, epithelia, and stroma) can be identified in classic triphasic Wilms' tumour histology.[14][42]
Two classification systems used, based on histology:[55]
COG: presence or absence of anaplasia.
SIOP: low-risk (completely necrotic, cystic, partially differentiated), intermediate-risk (histology that is not low-risk or high-risk), high-risk (blastemal, diffuse anaplastic).
Result
confirms the diagnosis with characteristic pathological appearances
genetic testing
Test
Patients with isolated Wilms' tumour, or those with Wilms' tumour and associated syndromes, may be tested for deletions of WT1 and other contiguous genes such as PAX6 by fluorescent in situ hybridisation (FISH).
Patients with clinical features suggestive of Beckwith-Wiedemann syndrome may be tested for a duplication of 11p15.5 by high-resolution chromosomal analysis and FISH.[43]
Result
deletions of WT1 and other contiguous genes
loss of heterozygosity (LOH) studies
Test
Positive LOH studies are associated with worse outcomes, and are performed on freshly frozen tumour tissue obtained by radical nephrectomy.[44]
Result
LOH at 16q and 1p
Use of this content is subject to our disclaimer