Approach
Hantavirus cardiopulmonary syndrome (HCPS) is a notifiable condition in some countries. A history of peridomestic exposure to rodents or cleaning rodent-infested enclosures is an epidemiological clue to diagnosing hantavirus infection.
HCPS infection is best understood as occurring in stages.[44]
Following virus exposure there is an asymptomatic incubation period of 9 to 33 days (median of 14 to 17 days, and up to 3 weeks after rodent bite).[28][29]
A prodromal non-specific viral illness follows with fever, headache, myalgias, and often prominent gastrointestinal (GI) symptoms.
During an early pulmonary syndrome phase there is increasing dyspnoea and hypoxaemia.
In the cardiopulmonary phase the patient is gravely ill with pulmonary oedema, thrombocytopenia, haemoconcentration, and cardiogenic shock.
In those survivors of the cardiopulmonary phase, there follows a diuresis phase with resolution of the pulmonary oedema. Convalescence may be prolonged.
Prodromal illness
Diagnosis is rarely made at this stage of illness due to non-specific symptoms. Prodromal viral illness symptoms including fever, headache, myalgia, and GI symptoms (anorexia, nausea, vomiting, diarrhoea, and abdominal pain) are usually present.[45] Upper respiratory tract symptoms (e.g., sore throat, nasal congestion, sneezing), are rarely described with hantavirus infection and would tend to exclude the diagnosis.[45] Epidemiological history of rodent infestation in or around the dwelling, and/or cleaning out of rodent-contaminated enclosed areas, are suggestive of an HCPS infection.
Clinically, the patient may be tachypnoeic, but oxygen saturations will be normal.
Investigations are often not performed at this stage, but if a full blood count (FBC) is done it may provide an early clue to the disease. Thrombocytopenia with a supporting epidemiology is suggestive of hantavirus infection.[46] The degree of thrombocytopenia may be prognostic of poor outcome.[5]
Enzyme-linked immunosorbent assay (ELISA) immunoglobulin (Ig) M-capture and IgG serologies for Sin Nombre virus (SNV) are ordered if the epidemiology and clinical presentation are suggestive of hantavirus infection.[47] By the time the symptoms are evident, patients uniformly have antiviral antibodies of IgM class and some have antibodies of the IgG class.
In Brazil, a recombinant nucleocapsid protein of Araraquara virus (ARQV) was obtained in Escherichia coli and has been successfully used as an antigen in an indirect ELISA for diagnosis of hantavirus disease and serological surveys.[48]
Early pulmonary phase
Progression of the disease results in increasing dyspnoea with low oxygen saturations.
All patients with respiratory symptoms should have a chest x-ray (CXR) and basic blood tests performed. CXR may be normal or suggestive of early interstitial oedema. The FBC will show thrombocytopenia with an elevated haemoglobin (Hb) and haematocrit (Hct) as evidence of haemoconcentration. There is an associated leukocytosis with juvenile forms (immunoblasts).[45] An immunoblast count >10% of the total lymphocyte count along with myelocytes, an elevated Hb, and thrombocytopenia (<150 x 10⁹/L [<150 x 10³/microlitre]) on FBC is highly suggestive of hantavirus infection.[49]
If the epidemiology, clinical presentation, and initial investigations support the possibility of hantavirus infection, then hantavirus serology should be requested (if not already done). Hantavirus-RNA detection by polymerase chain reaction (PCR) is also available, although still considered experimental.[50] High-level viraemia at presentation may be predictive of more severe disease.[51]
Neutralising antibodies are detectable in this phase, although this is an emerging test and is not routinely performed.[52]
Hantavirus isolation in cell culture is not a routine procedure for laboratory diagnosis; nevertheless, Andes virus (ANDV) has been isolated in cell culture from the blood of patients and from organs of fatal cases.[4]
Cardiopulmonary phase
Progression of the disease results in hypotension and pulmonary oedema.
Investigation with FBC, CXR, and arterial blood gas (ABG) are required. The FBC shows haemoconcentration, as indicated by an elevated Hb and Hct. This is a marker for capillary leak. CXR shows evidence of progressive non-cardiogenic pulmonary oedema (the heart size remains normal and pulmonary infiltrates ± pleural effusion may be present). [Figure caption and citation for the preceding image starts]: Bilateral fluffy pulmonary infiltrates in hantavirus pulmonary syndromeCDC Public Health Image Library (PHIL), Loren Ketai, MD [Citation ends].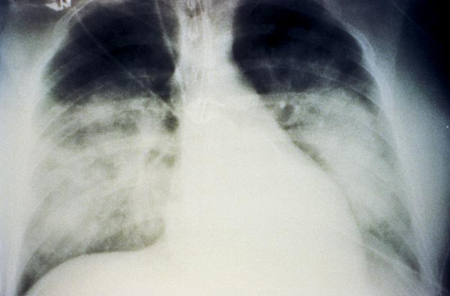 ABG shows a metabolic acidosis. Serum lactate should be performed, as elevated levels are a marker of poor outcome.
ABG shows a metabolic acidosis. Serum lactate should be performed, as elevated levels are a marker of poor outcome.
Once the cardiopulmonary phase begins, the disease can progress rapidly to cardiogenic shock and death and must be managed in an intensive care unit.[43] Cardiac evaluation is required. The ECG may show arrhythmias ranging from a sinus bradycardia to ventricular fibrillation, and an echocardiogram will show depressed cardiac ejection fraction. Haemodynamic measurement is recommended. During the cardiopulmonary phase, a decreased cardiac index and increased peripheral resistance are seen, distinguishing the shock from septic shock, which has a low systemic resistance and high cardiac output. Peripheral resistance and cardiac index are assessed using a flow-directed pulmonary artery catheter (Swan-Ganz catheter). A cardiac index of <2.5 L/minute/m² is one of the criteria for instituting extracorporeal membrane oxygenation.[44][53]
Lung biopsy may be performed either transbronchially at bronchoscopy or by video-assisted thoracoscopic surgery in patients with unexplained rapidly progressive pulmonary disease. In cases of HCPS it will show intra-alveolar oedema with an interstitial infiltrate of immunoblasts. There will be scant polymorphonuclear cells. Endothelial and alveolar lining cells are intact and appear normal. Immunohistochemical staining for hantavirus RNA is available as a research test through the US Centers for Disease Control and Prevention and will show diffuse endothelial cell staining.[53][54]
In South America, hantavirus serology detecting IgM-specific antibodies is the most used option for diagnosing cases of acute hantavirus infection. In addition to that, real-time reverse transcriptase PCR (RT-PCR) is able to determine the specific type of hantavirus causing the infection. The combination of a serological test, such as IgM ELISA, with RT-PCR is highly sensitive and represents a desirable approach to the laboratory diagnosis of HCPS.[55]
Diuresis phase
In survivors of the cardiopulmonary phase, there follows a diuresis phase with resolution of the pulmonary oedema. Convalescence may be prolonged.
Use of this content is subject to our disclaimer