Approach
An infant with a head tilt is not always obvious, as head control emerges over the first few months. Carers may notice a head tilt or tendency to look to one side immediately after birth, but in other cases, the asymmetry goes unrecognised for a few months. Alternatively, the primary care physician may be the first to notice a head tilt or rotation preference at the 2-month well child check. Cranial asymmetries, such as flattening of one occiput, may be present at birth or may not develop until the first few months of life. Early education and treatment is crucial for preventing further deformity.
History
Presence of a head tilt or cranial asymmetry should prompt questioning regarding birth history. Children with congenital muscular torticollis (CMT) have been found to have an increased incidence of complicated deliveries, such as requiring forceps or caesarean sections, breech positioning, and twin births (particularly twin A).
Sleeping position, feeding position, and use of other positioning devices (such as bouncy seats, infant carriers, floor entertainers) during the day should be investigated. These questions are important to determine whether the asymmetries are being perpetuated. For example, when the infant is placed in the same orientation in the crib resulting in more stimuli on one side, or when bottle feeding or carrying is restricted to one side, asymmetries can be perpetuated. It is important to enquire about supervised prone time during the day.
Carers should be asked about any abnormal eye movements or developmental concerns as these could indicate an ocular or neurological aetiology, respectively.
Examination
The resting posture of the infant should be observed. Typically, the infant's head is tilted to the side of the shortened sternocleidomastoid (SCM) muscle and rotated to the contralateral side.
The physician should passively rotate and tilt the head in both directions. The SCM may feel taut, and there may or may not be a palpable mass in the muscle. If a mass is present, it is usually only detectable during the first several months of life.
The ipsilateral shoulder may be observed to be elevated, and the associated upper trapezius muscle may be taut.
Infants typically have decreased active rotation to the affected side, whereas in unaffected children there is 100° of neck rotation bilaterally.
Head righting is often more difficult to the contralateral side.
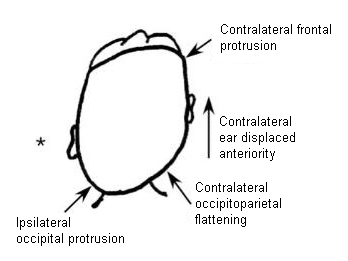
If plagiocephaly and craniofacial asymmetry are present, typical findings include:
Contralateral occipital flattening
Contralateral frontal protrusion
Ipsilateral temporal protrusion
Ipsilateral zygoma flattening
Anterior displacement of the contralateral ear
Inferior displacement of the ipsilateral orbit.[Figure caption and citation for the preceding image starts]: Vertex view of a head depicting typical findings of plagiocephaly associated with congenital muscular torticollis. Note the typical parallelogram shape due to asymmetrical external compressive forces and associated growth. *Denotes the side of the shortened sternocleidomastoid and resultant torticollisPrepared by Dr Joyce L. Oleszek; used with permission [Citation ends].
Eye movements should be evaluated, and hypertropia on the contralateral side should be sought. Suspicion of an ocular problem either by examination or by history warrants referral to an ophthalmologist.
A complete neurological examination should be performed, with any positive findings investigated further to rule out non-muscular aetiologies, with referral to a neurologist.
Hips should be evaluated for clicks or asymmetry in range of motion to rule out developmental dysplasia of the hip (DDH). A clear association has been demonstrated between DDH and CMT. It is possible for even an experienced examiner to miss DDH on physical examination alone; thus, imaging is recommended.[22] Referral to an orthopaedist should be made if abnormalities are found.
Imaging
A cervical spine x-ray is indicated in all infants with suspected CMT to rule out a vertebral anomaly.
A hip ultrasound should be obtained in children under the age of 6 months and an anteroposterior pelvic x-ray in children older than 6 months to rule out hip dysplasia if clinical examination reveals hip clicks, asymmetrical hip range of motion, or asymmetrical skin folds. In one study, the positive predictive value of clinical examinations for hip dysplasia was 52.6%.[23] The reported concurrence of CMT with hip dysplasia varies between 2% and 20%.[16][24][25][26]
A skull x-ray would be indicated to rule out craniosynostosis if plagiocephaly is noted but features are atypical of those seen in CMT.
If torticollis is associated with neurological symptoms or occurs intermittently with neurological symptoms, cranial/cervical spine MRI is indicated to rule out a posterior fossa or spinal cord tumour.
Use of this content is subject to our disclaimer