Approach
Diagnosis is made by assessing signs and symptoms, biochemical evidence of hyperthyroidism, and radioisotope scan with typical uptake and appearance.
History and physical
History of living in an iodine-deficient region should be sought. Onset of symptoms for toxic multinodular goitre (MNG) is more insidious and the symptoms less dramatic than for Graves' disease.[12] Younger patients are more likely to have typical symptoms of hyperthyroidism, such as hyperphagia, weight loss, sweating, heat intolerance, nervousness, palpitations, oligomenorrhoea, or hyperdefecation.
Older patients may have apathetic hyperthyroidism with mood change, weight loss, or atrial fibrillation alone.[5] The conduction system is slower in older people than in young people; therefore, tachycardia is less common and the ventricular rate in atrial fibrillation may not be rapid.
A goitre is usually present but can be small or non-palpable, particularly in older patients. Some patients present with symptoms of neck compression such as dysphagia, dyspnoea, or a choking sensation, but other causes need to be ruled out.[1] In severe cases of thoracic inlet obstruction, a Pemberton sign may be present (extension of arms over the head results in jugular venous distension and facial plethora).[23][24]
Physical findings may include warm moist skin, stare, lid lag, tremor, or proximal muscle weakness when hyperthyroidism is overt. Stigmata of Graves' disease, including exophthalmos and pretibial myxoedema, are absent.[3]
Tests
Thyroid-stimulating hormone (TSH) is the initial screening test. If TSH is suppressed, thyroid hormone levels (T4/T3) should be measured. The preferred tests are: free T4; and total T3 plus a measure of binding. Generally, free T4 level is elevated. Some patients may have sub-clinical hyperthyroidism with suppressed TSH and normal levels of thyroid hormones. T3 is elevated and T4 is usually high-normal in T3 toxicosis.
In the absence of stigmata of Graves’ disease or positive TSH receptor antibodies, thyroid scan and uptake are indicated when biochemical hyperthyroidism is confirmed. In toxic MNG, this shows multiple hot and cold areas consistent with areas of autonomy and suppression. I-123 is the preferred isotope.[25] Tc-99 pertechnetate scan is an alternative for imaging the thyroid, but there is a risk of false-positive images and uptake cannot be measured.[1] I-123 uptake is typically lower than for Graves' disease and is often within the normal range.
Thyroid ultrasound is not helpful for diagnosis, but may be used to further define any cold nodules found on a scan. Cold nodules >1 cm in diameter with suspicious ultrasonographic characteristics (such as more-tall-than-wide shape, irregular margins, microcalcifications, or marked hypoechogenicity) should be considered for further evaluation with fine needle biopsy.[1][26][27][28]
FBC may show non-specific anaemia or leukocytosis. Baseline WBC count is useful prior to starting antithyroid drugs. Mild neutropenia should not be regarded as a contraindication to the use of antithyroid drug therapy and hyperthyroidism typically normalises the neutrophil count.[29] Urea and electrolytes may show elevated LFTs or calcium. Elevated alkaline phosphatase is generally of bony origin, due to increased bone turnover. Most patients with hyperthyroidism will have elevated transaminases prior to initiating treatment and levels typically improve with antithyroid drug therapy.[30] Thyroid peroxidase antibodies are non-specific, but a positive result may support a diagnosis of Graves' disease. TSH receptor antibodies may be useful to distinguish toxic MNG from Graves' disease; third-generation TSH receptor antibody assays are highly sensitive and specific for Graves' disease.
An ECG may be required for suspected dysrhythmia. Occasionally a non-contrast CT scan of the neck is indicated to evaluate a large goitre with compressive symptoms, or as part of a pre-operative evaluation before thyroidectomy. [Figure caption and citation for the preceding image starts]: Thyroid scan showing variegated uptake in toxic multinodular goitreCourtesy of Dr Elizabeth Pearce; used with permission [Citation ends].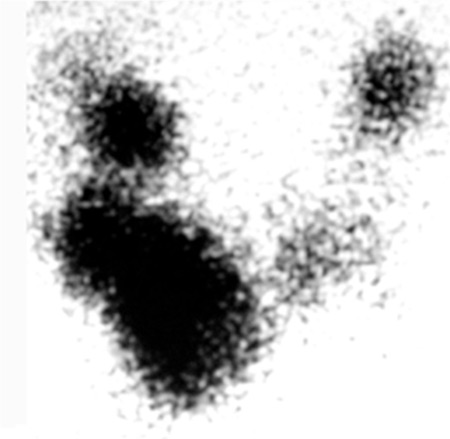 [Figure caption and citation for the preceding image starts]: Chest CT showing marked enlargement of the thyroid gland with an extensive intrathoracic component causing trachea compressionDias T et al. Acute airway obstruction due to benign multinodular goitre. BMJ Case Reports. 2019;12:e228095; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Chest CT showing marked enlargement of the thyroid gland with an extensive intrathoracic component causing trachea compressionDias T et al. Acute airway obstruction due to benign multinodular goitre. BMJ Case Reports. 2019;12:e228095; used with permission [Citation ends].
Use of this content is subject to our disclaimer