History and exam
Key diagnostic factors
common
presence of risk factors
Risk factors include: transplant recipients who are cytomegalovirus (CMV)-seronegative with a seropositive donor, transplant recipients who are CMV-seropositive, graft-versus-host disease, certain immunosuppressive drugs, AIDS, organ or haematopoietic stem cell transplant, acute illness in intensive care setting, and CMV infection in pregnancy (risk of congenital CMV disease in the newborn).
malaise
New or significant increase in malaise/fatigue is often the first symptom in solid-organ transplant (SOT)-related cytomegalovirus disease, and may not initially be accompanied by fever.[1]
fever
Fever is a common clinical presentation of cytomegalovirus disease in transplant recipients.[19]
diarrhoea
The most common organ-invasive symptom of cytomegalovirus disease in transplant recipients.[19]
nausea and vomiting
A common gastrointestinal tissue-invasive symptom of cytomegalovirus disease.[19]
visual floaters and blindness
abnormalities on fundoscopy
A fundoscopic examination is indicated in AIDS patients with CD4 T-cell count of <50 cells/microlitre. Transplant patients with visual complaints should be examined by fundoscopy to check for the presence of cytomegalovirus (CMV) retinitis.[37]
In the presence of CMV retinitis, fundoscopy will reveal areas of infarction, haemorrhage, peri-vascular sheathing, and retinal opacification.[Figure caption and citation for the preceding image starts]: Fundoscopy (left eye) showing area of CMV retinitis inferonasally involving the vascular arcades and the optic disc, associated with vasculitis and flame haemorrhagesAdapted from BMJ Case Reports 2009, copyright © 2009 by the BMJ Publishing Group Ltd [Citation ends].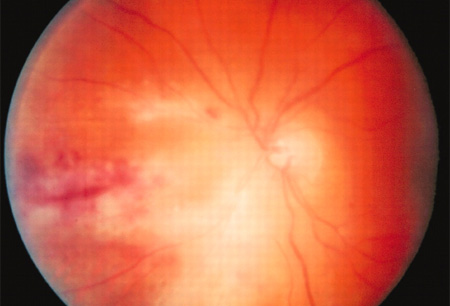
newborn: microcephaly
Microcephaly may be evident at antenatal ultrasound or at birth.
newborn: poor tone and motor function and abnormal head lag
Common signs of neurological involvement in the newborn.[10]
newborn: hearing loss
One of the most common clinical manifestations of congenital cytomegalovirus infection; may be suspected by the inability of the newborn to respond to sound and verbal stimuli.[10]
Other diagnostic factors
common
newborn: hepatosplenomegaly
Hepatosplenomegaly may be evident at antenatal ultrasound or at birth.
newborn: petechiae or purpura
Severe thrombocytopenia in the newborn may lead to multiple purpura and petechial lesions.[10]
uncommon
pain and weakness
Pain and weakness may indicate the presence of cytomegalovirus polyradiculopathy, especially in AIDS patients.
Risk factors
strong
CMV D+/R- status (donor CMV seropositive, recipient seronegative) in solid organ transplant recipients
Transmission of cytomegalovirus (CMV) through the allograft to the immunologically-naive transplant recipient is considered the most important risk factor for the development of CMV disease following solid organ transplantation.
Depending on the type of organ transplant, up to 90% of CMV-seronegative transplant recipients develop primary CMV disease if they receive organ allografts from CMV-seropositive donors.[18] The risk is highest in CMV D+/R- lung transplant recipients and relatively lower in CMV D+/R- kidney transplant recipients.[18][19]
CMV R+ (recipient seropositive) in transplant recipients
The re-activation of latent cytomegalovirus (CMV) is particularly common in recipients after allogeneic haematopoietic stem cell transplant, and in CMV-seropositive solid organ transplant recipients, particularly in patients who receive lymphocyte-depleting antibodies and patients who previously developed acute allograft rejection.[20]
CMV-seropositivity in allogeneic stem cell transplant recipients is one of the strongest risk factors for the development of CMV viraemia and disease after haematopoietic stem cell transplantation, in particular in patients developing graft-versus-host disease.[21]
type of immunosuppressive drugs
The overall net state of immunosuppression, which is partly due to the combined effects of immunosuppressive drugs, is a major risk factor for cytomegalovirus (CMV) disease in transplant recipients. In contrast, the impact of an individual immunosuppressive drug on the risk of CMV disease is variable.
High doses of corticosteroids, mycophenolate mofetil, anti-thymocyte globulin, and alemtuzumab have all been reported to significantly increase the risk of CMV disease in solid organ and haematopoietic stem cell transplant recipients.[22] These drugs impair the ability of patients to combat a re-activating CMV infection, thereby leading to uncontrolled viral replication and clinical disease. Recently, belatacept use has been associated with atypical manifestations and a high rate of end-organ disease.[23]
Sirolimus and everolimus have been associated with lower risk of CMV disease.[22][24][25]
AIDS
Patients with AIDS who have a CD4 T-cell count of <50 cells/microlitre are at highest risk of developing cytomegalovirus (CMV) retinitis and other organ-invasive CMV diseases.[2]
The use of antiretroviral therapy that is directed against HIV infection leads to immune reconstitution (illustrated by the recovery of CD4+ T cells) and significantly reduces the risk of CMV disease.
inflammatory bowel disease
In patients with Crohn's disease and ulcerative colitis, cytomegalovirus (CMV) is considered to be a cause of severe or refractory colitis, and it is associated with an increased incidence of complications. Older age and use of high doses of corticosteroids have been identified as risk factors for CMV colitis in patients with inflammatory bowel disease.[26]
acute illness in intensive care setting
In critically ill patients (e.g., those with sepsis), reactivation of latent cytomegalovirus (CMV) can occur due to a pro-inflammatory environment characterised by release of tumour necrosis factor-alpha in a condition called cytokine storm.
Even in critically ill patients with apparent normal immune function, CMV reactivation has been observed during periods of bacterial sepsis.[27]
newborn in CMV infection during pregnancy
Use of this content is subject to our disclaimer