Approach
The condition commonly presents with flushing and diarrhoea; other clinical features include wheeze, palpitations, telangiectasia, and abdominal pain. Classic facies and cardiac signs are features of examination. Diagnosis is confirmed by elevated levels of urinary 5-hydroxyindoleacetic acid (5-HIAA); chromogranin A is often elevated in the presence of liver metastases.[8]
History
Patients often describe having symptoms for many months prior to presentation. Onset is often insidious. The two most common symptoms are diarrhoea and flushing, while wheeze occurs less commonly.
Diarrhoea often follows no specific pattern and may initially be intermittent due to secretory factors. Often, diarrhoea is associated with crampy abdominal pain and urgency, and can occur during both day and night.
Flushing is characteristically described as a sudden onset of pink to red discolouration involving the face and upper trunk. This usually lasts a few minutes and can occur intermittently throughout the day. Triggers leading to flushing include stress, tyramine-containing foods (chocolate, bananas, walnuts), and alcohol.
Wheeze is caused by bronchial constriction mediated via tachykinins and bradykinins. This is more common in those with bronchial carcinoid tumours.
Examination
Classic facies of carcinoid syndrome consists of pink to red discoloration around the face and upper trunk. In patients with atypical flushing, which may last for several hours, telangiectasia and hypertrophy of the face may be seen.
Wheeze may be heard on auscultation of the chest. A raised jugular venous pressure and features of right heart failure may be present in patients with carcinoid heart disease related to carcinoid syndrome. Right-sided cardiac murmurs of tricuspid regurgitation and pulmonary stenosis may be heard on cardiovascular examination.
Abdominal examination may reveal hepatomegaly, which may be massive. On palpation of the abdomen, fixed masses, which are often related to desmoplastic reaction, may be palpated in the right iliac fossa. A desmoplastic reaction is characterised by the growth of dense fibrous tissue around the neoplasm.
Rarely, features related to pellagra, a vitamin deficiency disease caused by dietary lack of niacin (B3), may be seen; these include dermatitis (itchy erythematous skin lesions) and dementia/confusional state.
Investigations
Initial blood tests should include full blood count, metabolic panel, liver function tests, fasting gut hormone profile including chromogranin A and chromogranin B, and 24-hour urinary 5-HIAA.[12] A dual-phase staging CT scan of the chest, abdomen, and pelvis may be appropriate if any hormonal tests are abnormal. Endoscopy and bronchoscopy can be used to help identify the primary site of the tumour. Somatostatin receptor scintigraphy (octreoscan), a nuclear medicine imaging modality, should be considered in any patients with histologically proven neuroendocrine tumours (NETs) or in patients with suspected NETs and lesions identified on CT. Iodine I-123 meta-iodobenzylguanidine (MIBG) scintigraphy can be requested from a nuclear medicine department to identify areas of tumours through the take-up of MIBG. Octreotate positive emission tomography (PET) scan is a new modality, which appears to be more sensitive than octreoscan.[13][14][Figure caption and citation for the preceding image starts]: Iodine I 123 meta-iodobenzylguanidine (MIBG) uptake image showing multiple metastasesFrom the collection of Dr R. Srirajaskanthan and Dr M. Caplin; used with permission [Citation ends].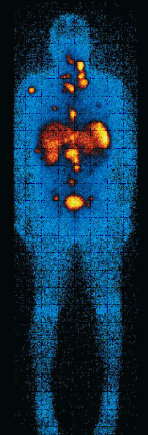 [Figure caption and citation for the preceding image starts]: CT scan showing multiple liver metastasesFrom the collection of Dr R. Srirajaskanthan and Dr M. Caplin; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: CT scan showing multiple liver metastasesFrom the collection of Dr R. Srirajaskanthan and Dr M. Caplin; used with permission [Citation ends].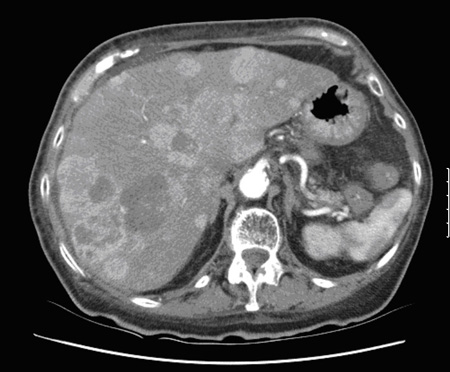
Use of this content is subject to our disclaimer