Thyroid cancer
- Overview
- Theory
- Diagnosis
- Management
- Follow up
- Resources
Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
papillary, follicular, or oncocytic
active surveillance or surgery (lobectomy or total thyroidectomy ± central neck dissection)
For patients with very low-risk tumours (e.g., unifocal papillary microcarcinomas [≤1 cm] with no evidence of extracapsular extension or lymph node metastases), active surveillance with ultrasound follow-up of the thyroid and neck lymph nodes every 6-12 months can be considered.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [59]National Institute for Health and Care Excellence. Thyroid cancer: assessment and management. Dec 2022 [internet publication]. https://www.nice.org.uk/guidance/ng230 [66]Tuttle RM, Alzahrani AS. Risk stratification in differentiated thyroid cancer: from detection to final follow-up. J Clin Endocrinol Metab. 2019 Mar 15;104(9):4087-100. https://academic.oup.com/jcem/article/104/9/4087/5380478 http://www.ncbi.nlm.nih.gov/pubmed/30874735?tool=bestpractice.com [69]European Society for Medical Oncology. Clinical practice guidelines - thyroid cancer. 2019 [internet publication]. https://www.esmo.org/guidelines/guidelines-by-topic/endocrine-and-neuroendocrine-cancers/thyroid-cancer [70]Saravana-Bawan B, Bajwa A, Paterson J, et al. Active surveillance of low-risk papillary thyroid cancer: a meta-analysis. Surgery. 2020 Jan;167(1):46-55. http://www.ncbi.nlm.nih.gov/pubmed/31526581?tool=bestpractice.com
Guidance does not routinely recommend fine-needle aspiration (FNA) for a cytological diagnosis on nodules less than 1 cm with low-risk features; however, this policy varies internationally, with some countries performing FNA and cytology for suspicious nodules before offering active surveillance.[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [71]Ito Y, Miyauchi A, Oda H. Low-risk papillary microcarcinoma of the thyroid: a review of active surveillance trials. Eur J Surg Oncol. 2018 Mar;44(3):307-15. https://www.ejso.com/article/S0748-7983(17)30370-0/fulltext http://www.ncbi.nlm.nih.gov/pubmed/28343733?tool=bestpractice.com
Active surveillance may be the preferred option in older patients and those at high surgical risk.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [69]European Society for Medical Oncology. Clinical practice guidelines - thyroid cancer. 2019 [internet publication]. https://www.esmo.org/guidelines/guidelines-by-topic/endocrine-and-neuroendocrine-cancers/thyroid-cancer
Transitioning to surgery during active surveillance is indicated if the patient requests surgery or there are clinical changes (e.g., new biopsy-proven lymph node metastases; distant metastases; invasion into recurrent laryngeal nerve, trachea, or oesophagus; radiological evidence of extrathyroidal extension; cancer growth by 3 mm in any dimension or a 50% volume increase).[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [71]Ito Y, Miyauchi A, Oda H. Low-risk papillary microcarcinoma of the thyroid: a review of active surveillance trials. Eur J Surg Oncol. 2018 Mar;44(3):307-15. https://www.ejso.com/article/S0748-7983(17)30370-0/fulltext http://www.ncbi.nlm.nih.gov/pubmed/28343733?tool=bestpractice.com
For all other thyroid cancers, surgery is generally recommended for initial treatment.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [59]National Institute for Health and Care Excellence. Thyroid cancer: assessment and management. Dec 2022 [internet publication]. https://www.nice.org.uk/guidance/ng230 [69]European Society for Medical Oncology. Clinical practice guidelines - thyroid cancer. 2019 [internet publication]. https://www.esmo.org/guidelines/guidelines-by-topic/endocrine-and-neuroendocrine-cancers/thyroid-cancer Total thyroidectomy is considered the standard surgical treatment. However, in patients with a tumour between 1 cm and 4 cm in diameter without extrathyroidal extension, and without clinical evidence of any lymph node metastases, lobectomy can be considered for the initial surgical procedure.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com It is important that patients understand that intraoperative findings during lobectomy may necessitate completion of a total thyroidectomy (completion thyroidectomy).[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
Surgery (e.g., total thyroidectomy or lobectomy) is required to confirm (histologically) a diagnosis of follicular or oncocytic carcinoma because FNA cytology does not reliably distinguish between follicular or oncocytic adenoma (benign) and carcinoma.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
If invasive follicular or oncocytic carcinoma is diagnosed following initial lobectomy, then subsequent completion thyroidectomy may be required depending on the invasiveness of the tumour.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
Completion thyroidectomy is required if patients have invasive follicular or oncocytic carcinoma that is: widely invasive (gross invasion of the thyroid gland with or without adjacent soft tissues and blood vessels), or encapsulated angioinvasive with involvement of ≥4 blood vessels.[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
Disease monitoring is typically preferred in a patient with invasive follicular or oncocytic carcinoma that is: minimally invasive (encapsulated tumour with microscopic capsular invasion and without vascular invasion), or is encapsulated angioinvasive with involvement of <4 blood vessels.[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
Complications of total thyroidectomy include an increased risk of recurrent laryngeal nerve damage or hypoparathyroidism.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx The risk of permanent hypoparathyroidism is higher for total than for subtotal thyroidectomy. The patient should be referred to an experienced surgeon.
Therapeutic central neck dissection for patients with clinically involved central nodes should accompany total thyroidectomy to provide clearance of disease from the central neck.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com Prophylactic central neck dissection is controversial.[69]European Society for Medical Oncology. Clinical practice guidelines - thyroid cancer. 2019 [internet publication]. https://www.esmo.org/guidelines/guidelines-by-topic/endocrine-and-neuroendocrine-cancers/thyroid-cancer In some centres it is recommended, but the reduction in locoregional recurrence is accompanied by an increased rate of post-operative adverse effects.[74]Chen L, Wu YH, Lee CH, et al. Prophylactic central neck dissection for papillary thyroid carcinoma with clinically uninvolved central neck lymph nodes: a systematic review and meta-analysis. World J Surg. 2018 Sep;42(9):2846-57. http://www.ncbi.nlm.nih.gov/pubmed/29488066?tool=bestpractice.com
TSH suppression
Additional treatment recommended for SOME patients in selected patient group
Total thyroidectomy necessitates thyroid hormone replacement therapy (e.g., levothyroxine).
As circulating thyroid-stimulating hormone (TSH) stimulates proliferation in normal thyrocytes and most thyroid cancer cells, TSH-suppressive doses of thyroid hormone therapy are used.[14]Cabanillas ME, McFadden DG, Durante C. Thyroid cancer. Lancet. 2016 Dec 3;388(10061):2783-95. http://www.ncbi.nlm.nih.gov/pubmed/27240885?tool=bestpractice.com
The use of thyroid hormone suppression should be based on initial risk of disease and ongoing risk assessment of disease status (see Diagnostic criteria for risk stratification). The lowest possible amount of thyroid hormone should be used.[72]Biondi B, Cooper DS. Thyroid hormone suppression therapy. Endocrinol Metab Clin North Am. 2019 Mar;48(1):227-37. http://www.ncbi.nlm.nih.gov/pubmed/30717904?tool=bestpractice.com
In patients with high-risk disease, maintaining a serum TSH level of <0.1 mIU/L is recommended.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com Maintaining a serum TSH level of <0.1 mIU/L (but not necessarily undetectable) is also recommended in patients with residual structural disease or a biochemically incomplete response if they are young or at low risk of complications such as exogenous subclinical hyperthyroidism.[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [72]Biondi B, Cooper DS. Thyroid hormone suppression therapy. Endocrinol Metab Clin North Am. 2019 Mar;48(1):227-37. http://www.ncbi.nlm.nih.gov/pubmed/30717904?tool=bestpractice.com
In patients with intermediate-risk disease, maintaining a serum TSH level of 0.1 to 0.5 mIU/L is recommended.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com
In patients with low-risk disease, serum TSH levels should be maintained in the low to normal range (0.5 to 2.0 mIU/L).[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [69]European Society for Medical Oncology. Clinical practice guidelines - thyroid cancer. 2019 [internet publication]. https://www.esmo.org/guidelines/guidelines-by-topic/endocrine-and-neuroendocrine-cancers/thyroid-cancer
Patients with low-risk disease who have undergone lobectomy may not require thyroid hormone replacement therapy if their serum TSH is maintained in a low to normal target range.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com
TSH-suppressive doses of thyroid replacement therapy may result in exogenous subclinical hyperthyroidism, which in turn can result in adverse outcomes such as osteoporosis, fractures, and cardiovascular disease, including atrial fibrillation.[72]Biondi B, Cooper DS. Thyroid hormone suppression therapy. Endocrinol Metab Clin North Am. 2019 Mar;48(1):227-37. http://www.ncbi.nlm.nih.gov/pubmed/30717904?tool=bestpractice.com Bone loss is of particular concern for TSH suppression in post-menopausal, non-oestrogen-treated women, but the effect of TSH suppression on fracture rate is unclear.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [73]Brancatella A, Marcocci C. TSH suppressive therapy and bone. Endocr Connect. 2020 Jul;9(7):R158-72. https://ec.bioscientifica.com/view/journals/ec/9/7/EC-20-0167.xml http://www.ncbi.nlm.nih.gov/pubmed/32567550?tool=bestpractice.com
Primary options
levothyroxine: consult specialist for guidance on dose
radioactive iodine therapy
Additional treatment recommended for SOME patients in selected patient group
Risk assessment (based on surgical and pathological findings) and assessment of post-operative disease status (including serum thyroglobulin [Tg] measurements and neck ultrasound) are required to guide selection of patients for radioactive iodine therapy.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [54]Webb RC, Howard RS, Stojadinovic A, et al. The utility of serum thyroglobulin measurement at the time of remnant ablation for predicting disease-free status in patients with differentiated thyroid cancer: a meta-analysis involving 3947 patients. J Clin Endocrinol Metab. 2012 Aug;97(8):2754-63. https://academic.oup.com/jcem/article/97/8/2754/2823340 http://www.ncbi.nlm.nih.gov/pubmed/22639291?tool=bestpractice.com [75]Tuttle RM, Ahuja S, Avram AM, et al. Controversies, consensus, and collaboration in the use of (131)I therapy in differentiated thyroid cancer: a joint statement from the American Thyroid Association, the European Association of Nuclear Medicine, the Society of Nuclear Medicine and Molecular Imaging, and the European Thyroid Association. Thyroid. 2019 Apr;29(4):461-70. https://www.liebertpub.com/doi/10.1089/thy.2018.0597 http://www.ncbi.nlm.nih.gov/pubmed/30900516?tool=bestpractice.com [76]Pacini F, Fuhrer D, Elisei R, et al. 2022 ETA consensus statement: what are the indications for post-surgical radioiodine therapy in differentiated thyroid cancer? Eur Thyroid J. 2022 Jan 1;11(1):e210046. https://etj.bioscientifica.com/view/journals/etj/11/1/ETJ-21-0046.xml http://www.ncbi.nlm.nih.gov/pubmed/34981741?tool=bestpractice.com
The use of radioactive iodine therapy is recommended following total thyroidectomy in patients with high-risk disease and in selected patients with intermediate-risk disease.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [76]Pacini F, Fuhrer D, Elisei R, et al. 2022 ETA consensus statement: what are the indications for post-surgical radioiodine therapy in differentiated thyroid cancer? Eur Thyroid J. 2022 Jan 1;11(1):e210046. https://etj.bioscientifica.com/view/journals/etj/11/1/ETJ-21-0046.xml http://www.ncbi.nlm.nih.gov/pubmed/34981741?tool=bestpractice.com
Radioactive iodine therapy is not routinely recommended for patients with low-risk disease, but features that impact on recurrence risk, disease follow-up implications, and patient preferences should be considered.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [77]Leboulleux S, Bournaud C, Chougnet CN, et al. Thyroidectomy without radioiodine in patients with low-risk thyroid cancer. N Engl J Med. 2022 Mar 10;386(10):923-32. https://www.nejm.org/doi/10.1056/NEJMoa2111953 http://www.ncbi.nlm.nih.gov/pubmed/35263518?tool=bestpractice.com
Selecting the optimal dose of therapeutic radioactive iodine can be challenging and should be based on risk assessment, and individualised (e.g., guided by patient factors and treatment goal).[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [75]Tuttle RM, Ahuja S, Avram AM, et al. Controversies, consensus, and collaboration in the use of (131)I therapy in differentiated thyroid cancer: a joint statement from the American Thyroid Association, the European Association of Nuclear Medicine, the Society of Nuclear Medicine and Molecular Imaging, and the European Thyroid Association. Thyroid. 2019 Apr;29(4):461-70. https://www.liebertpub.com/doi/10.1089/thy.2018.0597 http://www.ncbi.nlm.nih.gov/pubmed/30900516?tool=bestpractice.com [76]Pacini F, Fuhrer D, Elisei R, et al. 2022 ETA consensus statement: what are the indications for post-surgical radioiodine therapy in differentiated thyroid cancer? Eur Thyroid J. 2022 Jan 1;11(1):e210046. https://etj.bioscientifica.com/view/journals/etj/11/1/ETJ-21-0046.xml http://www.ncbi.nlm.nih.gov/pubmed/34981741?tool=bestpractice.com Consult local guidance.
Increased thyroid-stimulating hormone (TSH) levels are required to induce radioactive iodine uptake in thyroid cells.[76]Pacini F, Fuhrer D, Elisei R, et al. 2022 ETA consensus statement: what are the indications for post-surgical radioiodine therapy in differentiated thyroid cancer? Eur Thyroid J. 2022 Jan 1;11(1):e210046. https://etj.bioscientifica.com/view/journals/etj/11/1/ETJ-21-0046.xml http://www.ncbi.nlm.nih.gov/pubmed/34981741?tool=bestpractice.com Administration of exogenous recombinant human TSH (rhTSH) is the preferred method of preparation for radioactive iodine therapy for most patients.[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
Following radioactive iodine therapy, a whole-body radioactive iodine scan should be obtained to stage the disease and document the radioactive iodine avidity of any structural lesions.[78]Gulec SA, Ahuja S, Avram AM, et al. A joint statement from the American Thyroid Association, the European Association of Nuclear Medicine, the European Thyroid Association, the Society of Nuclear Medicine and Molecular Imaging on current diagnostic and theranostic approaches in the management of thyroid cancer. Thyroid. 2021 Jul;31(7):1009-19. https://www.liebertpub.com/doi/10.1089/thy.2020.0826 http://www.ncbi.nlm.nih.gov/pubmed/33789450?tool=bestpractice.com
Use of a 'diagnostic' radioactive iodine scan following surgery but before radioactive iodine therapy is controversial.[75]Tuttle RM, Ahuja S, Avram AM, et al. Controversies, consensus, and collaboration in the use of (131)I therapy in differentiated thyroid cancer: a joint statement from the American Thyroid Association, the European Association of Nuclear Medicine, the Society of Nuclear Medicine and Molecular Imaging, and the European Thyroid Association. Thyroid. 2019 Apr;29(4):461-70.
https://www.liebertpub.com/doi/10.1089/thy.2018.0597
http://www.ncbi.nlm.nih.gov/pubmed/30900516?tool=bestpractice.com
[76]Pacini F, Fuhrer D, Elisei R, et al. 2022 ETA consensus statement: what are the indications for post-surgical radioiodine therapy in differentiated thyroid cancer? Eur Thyroid J. 2022 Jan 1;11(1):e210046.
https://etj.bioscientifica.com/view/journals/etj/11/1/ETJ-21-0046.xml
http://www.ncbi.nlm.nih.gov/pubmed/34981741?tool=bestpractice.com
A diagnostic radioactive iodine scan may yield information relevant to clinical decision-making in selected patients only.[78]Gulec SA, Ahuja S, Avram AM, et al. A joint statement from the American Thyroid Association, the European Association of Nuclear Medicine, the European Thyroid Association, the Society of Nuclear Medicine and Molecular Imaging on current diagnostic and theranostic approaches in the management of thyroid cancer. Thyroid. 2021 Jul;31(7):1009-19.
https://www.liebertpub.com/doi/10.1089/thy.2020.0826
http://www.ncbi.nlm.nih.gov/pubmed/33789450?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: Increased uptake of radioiodine in both pulmonary fields and the mediastinum due to miliary lung metastasis from papillary thyroid carcinomaGkountouvas A, Chatjimarkou F, Thomas D, et al. Miliary lung metastasis due to papillary thyroid carcinoma. BMJ Case Reports. 2009; doi:10.1136/bcr.06.2008.0322 [Citation ends].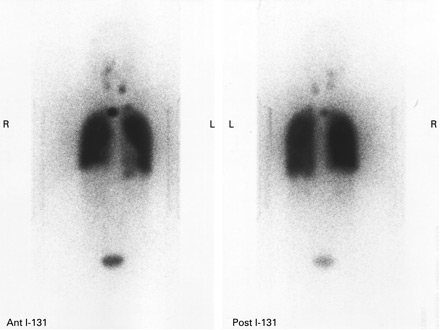
observation and surveillance ± surgery ± radioactive iodine therapy ± directed local therapies (e.g., external beam radiotherapy, thermal ablation)
The risk of recurrence is determined at time of diagnosis and re-evaluated as a continuum in response to early therapies.[66]Tuttle RM, Alzahrani AS. Risk stratification in differentiated thyroid cancer: from detection to final follow-up. J Clin Endocrinol Metab. 2019 Mar 15;104(9):4087-100. https://academic.oup.com/jcem/article/104/9/4087/5380478 http://www.ncbi.nlm.nih.gov/pubmed/30874735?tool=bestpractice.com Serum thyroglobulin assays and neck ultrasound are the mainstays of differentiated thyroid cancer follow-up.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [69]European Society for Medical Oncology. Clinical practice guidelines - thyroid cancer. 2019 [internet publication]. https://www.esmo.org/guidelines/guidelines-by-topic/endocrine-and-neuroendocrine-cancers/thyroid-cancer
Recurrence may be biochemical or structural.
Management of patients who develop biochemical recurrence (i.e., rising or newly elevated thyroglobulin levels), without evidence of structural disease, comprises observation and surveillance with appropriate imaging studies performed at time intervals guided by the thyroglobulin doubling time.[79]Scharpf J, Tuttle M, Wong R, et al. Comprehensive management of recurrent thyroid cancer: an American Head and Neck Society consensus statement. Head Neck. 2016 Dec;38(12):1862-9. https://onlinelibrary.wiley.com/doi/10.1002/hed.24513 http://www.ncbi.nlm.nih.gov/pubmed/27717219?tool=bestpractice.com
Patients with suspected structural neck recurrence (biopsy-proven persistent or recurrent disease) may require additional therapies or may be managed with observation and serial cross-sectional imaging (e.g., contrast-enhanced computed tomography [CT] or magnetic resonance imaging [MRI]) at a frequency sufficient to identify clinically significant disease progression.[79]Scharpf J, Tuttle M, Wong R, et al. Comprehensive management of recurrent thyroid cancer: an American Head and Neck Society consensus statement. Head Neck. 2016 Dec;38(12):1862-9. https://onlinelibrary.wiley.com/doi/10.1002/hed.24513 http://www.ncbi.nlm.nih.gov/pubmed/27717219?tool=bestpractice.com Recurrent structural disease that measures 8-10 mm or larger on anatomical imaging in the central and lateral neck, respectively, is considered for revision surgery.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com [79]Scharpf J, Tuttle M, Wong R, et al. Comprehensive management of recurrent thyroid cancer: an American Head and Neck Society consensus statement. Head Neck. 2016 Dec;38(12):1862-9. https://onlinelibrary.wiley.com/doi/10.1002/hed.24513 http://www.ncbi.nlm.nih.gov/pubmed/27717219?tool=bestpractice.com
Metastases are observed most frequently in patients with aggressive histological subtypes, and may occur in up to 10% of patients with differentiated thyroid cancer.[69]European Society for Medical Oncology. Clinical practice guidelines - thyroid cancer. 2019 [internet publication]. https://www.esmo.org/guidelines/guidelines-by-topic/endocrine-and-neuroendocrine-cancers/thyroid-cancer [80]Tumino D, Frasca F, Newbold K. Updates on the management of advanced, metastatic, and radioiodine refractory differentiated thyroid cancer. Front Endocrinol (Lausanne). 2017 Nov 20;8:312. https://www.frontiersin.org/articles/10.3389/fendo.2017.00312/full http://www.ncbi.nlm.nih.gov/pubmed/29209273?tool=bestpractice.com For the management of metastatic differentiated thyroid cancer, the American Thyroid Association recommends a preferred hierarchy of surgical excision of locoregional disease, radioactive iodine therapy for radioactive iodine-responsive disease (with thyroid-stimulating hormone [TSH]-suppressive therapy), directed local therapies (e.g., external beam radiotherapy, thermal ablation), and systemic therapy with kinase inhibitors.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com
For patients with stable or slowly progressive asymptomatic metastatic disease, TSH-suppressive thyroid hormone therapy alone can be used.[1]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133. https://www.liebertpub.com/doi/10.1089/thy.2015.0020 http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com
If distant metastases are radioactive iodine-responsive, radioactive iodine therapy is repeated every 6-12 months depending on rate of growth and response.[81]Verburg FA, Hänscheid H, Luster M. Radioactive iodine (RAI) therapy for metastatic differentiated thyroid cancer. Best Pract Res Clin Endocrinol Metab. 2017 Jun;31(3):279-90. http://www.ncbi.nlm.nih.gov/pubmed/28911724?tool=bestpractice.com As tumours progress, they may lose their ability to concentrate radioactive iodine.[33]Fugazzola L, Elisei R, Fuhrer D, et al. 2019 European Thyroid Association guidelines for the treatment and follow-up of advanced radioiodine-refractory thyroid cancer. Eur Thyroid J. 2019 Oct;8(5):227-45. https://etj.bioscientifica.com/view/journals/etj/8/5/ETJ502229.xml http://www.ncbi.nlm.nih.gov/pubmed/31768334?tool=bestpractice.com
targeted therapy
Additional treatment recommended for SOME patients in selected patient group
Treatment with kinase inhibitors, or other targeted therapies, may be considered for patients with progressive differentiated thyroid cancer who are not suitable for or not responsive to local treatment (including surgery and radioactive iodine therapy).
Genetic testing to identify potential actionable mutations/alterations (e.g., NTRK, BRAF, RET, mismatch repair deficiency [dMMR], microsatellite instability [MSI], tumour mutational burden [TMB]) is recommended prior to initiating therapy.[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [46]Filetti S, Durante C, Hartl DM, et al. ESMO clinical practice guideline update on the use of systemic therapy in advanced thyroid cancer. Ann Oncol. 2022 Jul;33(7):674-84. https://www.annalsofoncology.org/article/S0923-7534(22)00694-9/fulltext http://www.ncbi.nlm.nih.gov/pubmed/35491008?tool=bestpractice.com [82]Shonka DC Jr, Ho A, Chintakuntlawar AV, et al. American Head and Neck Society Endocrine Surgery Section and International Thyroid Oncology Group consensus statement on mutational testing in thyroid cancer: defining advanced thyroid cancer and its targeted treatment. Head Neck. 2022 Jun;44(6):1277-300. http://www.ncbi.nlm.nih.gov/pubmed/35274388?tool=bestpractice.com
If systemic therapy is indicated, the following kinase inhibitors are recommended first-line options: lenvatinib or sorafenib.[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
Alternative kinase inhibitors that may be considered include: cabozantinib (if progression occurs after lenvatinib and/or sorafenib); larotrectinib or entrectinib or repotrectinib (for NTRK gene fusion-positive advanced solid tumours); selpercatinib or pralsetinib (for RET gene fusion-positive tumours).[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
Targeted therapies that may be considered for patients with unresectable recurrent or metastatic solid tumours that have progressed following prior treatment with no satisfactory alternative treatment options, include: pembrolizumab (a programmed death receptor-1 [PD-1]-blocking monoclonal antibody for patients with TMB-high [≥10 mutations/megabase] tumours, or MSI-high or dMMR tumours); or dabrafenib plus trametinib (for patients with BRAF V600E mutation).[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
The optimal sequence of systemic therapy in this setting is unclear. Decision-making should be based on factors including expected treatment response, drug safety profile, and patient preference.
See local specialist protocol for dosing guidelines.
Primary options
sorafenib
OR
lenvatinib
Secondary options
cabozantinib
OR
larotrectinib
OR
entrectinib
OR
repotrectinib
OR
selpercatinib
OR
pralsetinib
Tertiary options
pembrolizumab
OR
dabrafenib
and
trametinib
anaplastic
surgery + chemoradiation
Anaplastic thyroid cancer is usually diagnosed at an advanced stage (often with distant metastases), displays extremely aggressive behaviour, and is associated with a very poor prognosis.[13]Bible KC, Kebebew E, Brierley J, et al. 2021 American Thyroid Association guidelines for management of patients with anaplastic thyroid cancer. Thyroid. 2021 Mar;31(3):337-86. https://www.liebertpub.com/doi/10.1089/thy.2020.0944 http://www.ncbi.nlm.nih.gov/pubmed/33728999?tool=bestpractice.com [69]European Society for Medical Oncology. Clinical practice guidelines - thyroid cancer. 2019 [internet publication]. https://www.esmo.org/guidelines/guidelines-by-topic/endocrine-and-neuroendocrine-cancers/thyroid-cancer
Early multidisciplinary involvement including the palliative care team is important to support patient decision-making.[13]Bible KC, Kebebew E, Brierley J, et al. 2021 American Thyroid Association guidelines for management of patients with anaplastic thyroid cancer. Thyroid. 2021 Mar;31(3):337-86. https://www.liebertpub.com/doi/10.1089/thy.2020.0944 http://www.ncbi.nlm.nih.gov/pubmed/33728999?tool=bestpractice.com Determining the extent of disease and assessing for mutations influences the treatment options (including eligibility for clinical trials) and goals of care.[13]Bible KC, Kebebew E, Brierley J, et al. 2021 American Thyroid Association guidelines for management of patients with anaplastic thyroid cancer. Thyroid. 2021 Mar;31(3):337-86. https://www.liebertpub.com/doi/10.1089/thy.2020.0944 http://www.ncbi.nlm.nih.gov/pubmed/33728999?tool=bestpractice.com
Combining multiple therapeutic modalities (surgery, radiotherapy, systemic therapy [chemotherapy, targeted therapy]) is the most effective approach to treating anaplastic thyroid cancer, but needs to be individualised to optimally balance risks and benefits.
Radioactive iodine therapy is not used because anaplastic tumours do not take up radioiodine.[13]Bible KC, Kebebew E, Brierley J, et al. 2021 American Thyroid Association guidelines for management of patients with anaplastic thyroid cancer. Thyroid. 2021 Mar;31(3):337-86. https://www.liebertpub.com/doi/10.1089/thy.2020.0944 http://www.ncbi.nlm.nih.gov/pubmed/33728999?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
If possible a total thyroidectomy is done. Determining whether a patient is a candidate for surgery depends on the tumour's resectability, extent of local invasion, need for urgent tracheostomy, presence of distant metastases, and the patient's performance status and treatment goals.[13]Bible KC, Kebebew E, Brierley J, et al. 2021 American Thyroid Association guidelines for management of patients with anaplastic thyroid cancer. Thyroid. 2021 Mar;31(3):337-86. https://www.liebertpub.com/doi/10.1089/thy.2020.0944 http://www.ncbi.nlm.nih.gov/pubmed/33728999?tool=bestpractice.com Thyroid hormone replacement is required post-total thyroidectomy.
Regardless of the surgical status, radiotherapy should be considered early in the treatment of anaplastic thyroid cancer.[83]Rao SN, Smallridge RC. Anaplastic thyroid cancer: an update. Best Pract Res Clin Endocrinol Metab. 2022 May 27;101678. http://www.ncbi.nlm.nih.gov/pubmed/35668021?tool=bestpractice.com
Chemotherapy with paclitaxel, docetaxel, or combined treatments (e.g., carboplatin/paclitaxel, docetaxel/doxorubicin) is associated with very low response rates and significant toxicities. Chemotherapy may, however, be considered for its radiosensitising effect when combined with radiotherapy, or as a bridge to targeted therapy by patients awaiting results of molecular profiling.[13]Bible KC, Kebebew E, Brierley J, et al. 2021 American Thyroid Association guidelines for management of patients with anaplastic thyroid cancer. Thyroid. 2021 Mar;31(3):337-86. https://www.liebertpub.com/doi/10.1089/thy.2020.0944 http://www.ncbi.nlm.nih.gov/pubmed/33728999?tool=bestpractice.com
See local specialist protocol for chemotherapy dosing guidelines.
Primary options
paclitaxel
OR
docetaxel
OR
paclitaxel
and
carboplatin
OR
docetaxel
and
doxorubicin
targeted therapy
Additional treatment recommended for SOME patients in selected patient group
Use of targeted therapy in patients with anaplastic thyroid cancer depends on the results of genetic testing.[13]Bible KC, Kebebew E, Brierley J, et al. 2021 American Thyroid Association guidelines for management of patients with anaplastic thyroid cancer. Thyroid. 2021 Mar;31(3):337-86. https://www.liebertpub.com/doi/10.1089/thy.2020.0944 http://www.ncbi.nlm.nih.gov/pubmed/33728999?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [46]Filetti S, Durante C, Hartl DM, et al. ESMO clinical practice guideline update on the use of systemic therapy in advanced thyroid cancer. Ann Oncol. 2022 Jul;33(7):674-84. https://www.annalsofoncology.org/article/S0923-7534(22)00694-9/fulltext http://www.ncbi.nlm.nih.gov/pubmed/35491008?tool=bestpractice.com [84]Maniakas A, Zafereo M, Cabanillas ME. Anaplastic thyroid cancer: new horizons and challenges. Endocrinol Metab Clin North Am. 2022 Jun;51(2):391-401. http://www.ncbi.nlm.nih.gov/pubmed/35662448?tool=bestpractice.com [85]Wang JR, Zafereo ME, Dadu R, et al. Complete surgical resection following neoadjuvant dabrafenib plus trametinib in BRAF(V600E)-mutated anaplastic thyroid carcinoma. Thyroid. 2019 Aug;29(8):1036-43. https://pmc.ncbi.nlm.nih.gov/articles/PMC6707029 http://www.ncbi.nlm.nih.gov/pubmed/31319771?tool=bestpractice.com
Dabrafenib plus trametinib: may be considered prior to surgery (to improve resectability) in patients with the BRAF V600E mutation and locoregional disease.
Larotrectinib or entrectinib or repotrectinib: for patients with NTRK gene fusion-positive advanced solid tumours.
Selpercatinib or pralsetinib: for patients with RET gene fusion-positive tumours.
Immunotherapy; for example, pembrolizumab, for patients with tumour mutational burden-high (TMB-H; ≥10 mutations/megabase) tumours.
See local specialist protocol for dosing guidelines.
Primary options
dabrafenib
and
trametinib
OR
larotrectinib
OR
entrectinib
OR
repotrectinib
OR
selpercatinib
OR
pralsetinib
Secondary options
pembrolizumab
medullary
surgery
Surgery for patients with sporadic or hereditary medullary thyroid cancer is total thyroidectomy and central compartment lymph node dissection, the extent of which depends on the serum calcitonin levels and ultrasound findings.[4]Wells SA Jr, Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015 Jun;25(6):567-610. https://www.liebertpub.com/doi/10.1089/thy.2014.0335 http://www.ncbi.nlm.nih.gov/pubmed/25810047?tool=bestpractice.com [53]Viola D, Elisei R. Management of medullary thyroid cancer. Endocrinol Metab Clin North Am. 2019 Mar;48(1):285-301. http://www.ncbi.nlm.nih.gov/pubmed/30717909?tool=bestpractice.com [69]European Society for Medical Oncology. Clinical practice guidelines - thyroid cancer. 2019 [internet publication]. https://www.esmo.org/guidelines/guidelines-by-topic/endocrine-and-neuroendocrine-cancers/thyroid-cancer [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx
thyroid hormone replacement
Additional treatment recommended for SOME patients in selected patient group
Thyroid hormone replacement (e.g., levothyroxine) is required after total thyroidectomy to maintain serum thyroid stimulating hormone (TSH) levels in the euthyroid range.[4]Wells SA Jr, Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015 Jun;25(6):567-610. https://www.liebertpub.com/doi/10.1089/thy.2014.0335 http://www.ncbi.nlm.nih.gov/pubmed/25810047?tool=bestpractice.com
Medullary thyroid cancer is not TSH-sensitive; therefore, suppressive doses of TSH are not required.
Primary options
levothyroxine: consult specialist for guidance on dose
surgery ± external beam radiotherapy ± focal treatments
Recurrences are treated with additional surgery, plus external beam radiotherapy if local control cannot be achieved.[86]Hadoux J, Pacini F, Tuttle RM, et al. Management of advanced medullary thyroid cancer. Lancet Diabetes Endocrinol. 2016 Jan;4(1):64-71. http://www.ncbi.nlm.nih.gov/pubmed/26608066?tool=bestpractice.com
In metastatic disease, surgery may be indicated for patients in whom a single or a few metastases are located in the brain, lungs, or liver.[86]Hadoux J, Pacini F, Tuttle RM, et al. Management of advanced medullary thyroid cancer. Lancet Diabetes Endocrinol. 2016 Jan;4(1):64-71. http://www.ncbi.nlm.nih.gov/pubmed/26608066?tool=bestpractice.com Focal treatments including external beam radiotherapy, stereotactic radiosurgery, radiofrequency ablation, or chemoembolisation are used depending on the site of metastases.[4]Wells SA Jr, Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015 Jun;25(6):567-610. https://www.liebertpub.com/doi/10.1089/thy.2014.0335 http://www.ncbi.nlm.nih.gov/pubmed/25810047?tool=bestpractice.com [86]Hadoux J, Pacini F, Tuttle RM, et al. Management of advanced medullary thyroid cancer. Lancet Diabetes Endocrinol. 2016 Jan;4(1):64-71. http://www.ncbi.nlm.nih.gov/pubmed/26608066?tool=bestpractice.com
targeted therapy
Additional treatment recommended for SOME patients in selected patient group
Kinase inhibitors have produced high response rates in patients with metastatic medullary thyroid cancer.[86]Hadoux J, Pacini F, Tuttle RM, et al. Management of advanced medullary thyroid cancer. Lancet Diabetes Endocrinol. 2016 Jan;4(1):64-71. http://www.ncbi.nlm.nih.gov/pubmed/26608066?tool=bestpractice.com
The multikinase inhibitors cabozantinib and vandetanib are recommended for first-line systemic therapy for patients with progressive, metastatic medullary thyroid cancer.[4]Wells SA Jr, Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015 Jun;25(6):567-610. https://www.liebertpub.com/doi/10.1089/thy.2014.0335 http://www.ncbi.nlm.nih.gov/pubmed/25810047?tool=bestpractice.com [37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [46]Filetti S, Durante C, Hartl DM, et al. ESMO clinical practice guideline update on the use of systemic therapy in advanced thyroid cancer. Ann Oncol. 2022 Jul;33(7):674-84. https://www.annalsofoncology.org/article/S0923-7534(22)00694-9/fulltext http://www.ncbi.nlm.nih.gov/pubmed/35491008?tool=bestpractice.com [82]Shonka DC Jr, Ho A, Chintakuntlawar AV, et al. American Head and Neck Society Endocrine Surgery Section and International Thyroid Oncology Group consensus statement on mutational testing in thyroid cancer: defining advanced thyroid cancer and its targeted treatment. Head Neck. 2022 Jun;44(6):1277-300. http://www.ncbi.nlm.nih.gov/pubmed/35274388?tool=bestpractice.com
The RET inhibitors selpercatinib and pralsetinib are recommended for patients with recurrent or metastatic RET-mutated medullary thyroid cancer.[37]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: thyroid carcinoma [internet publication]. https://www.nccn.org/professionals/physician_gls/default.aspx [46]Filetti S, Durante C, Hartl DM, et al. ESMO clinical practice guideline update on the use of systemic therapy in advanced thyroid cancer. Ann Oncol. 2022 Jul;33(7):674-84. https://www.annalsofoncology.org/article/S0923-7534(22)00694-9/fulltext http://www.ncbi.nlm.nih.gov/pubmed/35491008?tool=bestpractice.com
See local specialist protocol for dosing guidelines.
Primary options
cabozantinib
OR
vandetanib
Secondary options
selpercatinib
OR
pralsetinib
thyroid hormone replacement
Additional treatment recommended for SOME patients in selected patient group
Thyroid hormone replacement (e.g., levothyroxine) is required after total thyroidectomy to maintain serum thyroid stimulating hormone (TSH) levels in the euthyroid range.[4]Wells SA Jr, Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015 Jun;25(6):567-610. https://www.liebertpub.com/doi/10.1089/thy.2014.0335 http://www.ncbi.nlm.nih.gov/pubmed/25810047?tool=bestpractice.com
Medullary thyroid cancer is not TSH-sensitive; therefore, suppressive doses of TSH are not required.
Primary options
levothyroxine: consult specialist for guidance on dose
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer