Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
initial surveillance endoscopy + polyp excision
Small intestinal surveillance is recommended for all patients who meet the diagnostic criteria. This may be performed using video capsule endoscopy (VCE) or magnetic resonance enterography (MRE).
Guidelines differ with regard to the size threshold at which asymptomatic polyps of the small bowel should be removed, although all concur that any symptomatic polyps should be excised regardless of size. US guidelines recommend removal of asymptomatic polyps ≥10 millimetres in diameter, whereas European guidelines recommend a higher threshold of >15-20 millimetres.[13][14][19][20][22][33] Polypectomy is achieved via upper endoscopy or single or double balloon enteroscopy depending on the location of polyps. One series of 34 patients with small bowel hamartomatous polyposis found that double balloon enteroscopy was successful in more than 80% of patients and had an acceptable margin of safety.[39] Surgery may be required in the presence of neoplasia, or if polyp size or number preclude endoscopic removal. It may also be required in patients with intussusception or small bowel obstruction. Some authorities recommend an attempt to clear the small intestine of polyps during laparotomy by means of intraoperative endoscopy with polypectomy or, for larger polyps, by means of enterotomy. This aggressive approach to the diagnosis and resection of small bowel polyps ('clean sweep') has been associated with a longer interval between subsequent surgeries and a decrease in total operations.[14][35][36][37]
There are limited data to advise on the size of polyps which merit polypectomy in the stomach or colon.[13] The US Multi-Society Task Force on Colorectal Cancer is the only organisation to provide a specific recommendation, advising removal of polyps >5 millimetres in diameter and an attempt to remove all polyps if endoscopically feasible.[14] Colectomy is sometimes necessary and should be considered if colonoscopic management is difficult and especially if neoplastic change is found in colonic polyps.[4][Figure caption and citation for the preceding image starts]: Small bowel hamartomatous polyp identified on capsule endoscopyFrom the collection of Dr Carol A. Burke, used with permission [Citation ends].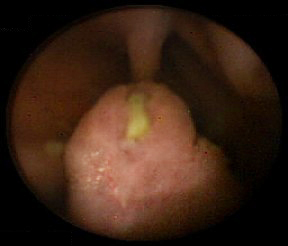 [Figure caption and citation for the preceding image starts]: Polypoid mass in the small bowelFrom the collection of Dr James Church, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Polypoid mass in the small bowelFrom the collection of Dr James Church, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Characteristic serosal dimpling resulting from a pedunculated hamartoma in the small bowel of a patient with PJSFrom the collection of Dr James Church, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Characteristic serosal dimpling resulting from a pedunculated hamartoma in the small bowel of a patient with PJSFrom the collection of Dr James Church, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Intra-operative endoscopyFrom the collection of Dr James Church, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Intra-operative endoscopyFrom the collection of Dr James Church, used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Hamartomatous polyp harvest following 'clean sweep'From the collection of Dr James Church, used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Hamartomatous polyp harvest following 'clean sweep'From the collection of Dr James Church, used with permission [Citation ends].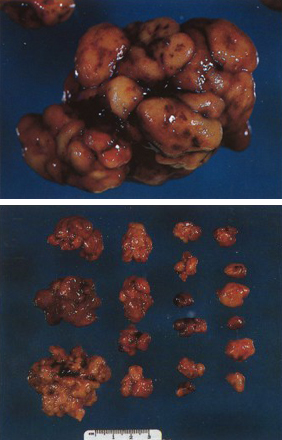
ongoing gastrointestinal surveillance ± polyp excision
Endoscopic surveillance is recommended to minimise the risk of complications such as obstruction, bleeding, or cancer. However, data are limited and the outcome on cancer incidence or mortality is unknown.
Surveillance protocols are determined by the risk of gastrointestinal cancer, based upon the presence, number, and size of polyps at index endoscopy; age and family history are also considerations.
Video capsule endoscopy (VCE) or magnetic resonance enterography (MRE) of the small bowel should begin by age 8 years (or earlier if the patient is symptomatic).[14][19][20][33] Capsule endoscopy is safe to use in individuals with PJS and small bowel polyposis who do not have obstructive symptoms. If a concern for capsule retention is present, a patency capsule should be utilised. If no polyps are found at the initial examination, US guidelines recommend that small bowel surveillance should resume at age 18 years and continue every 2-3 years throughout life, whereas European guidelines advise repeating it every 3 years from the outset.[13][14][19][20][22][33]
Oesophagogastroduodenoscopy (OGD) and colonoscopy to look for upper gastrointestinal and colorectal polyps should be done by age 8 years. If polyps are found, both examinations are repeated every 3 years; if no polyps are detected, a subsequent baseline examination is conducted at age 18 years, and every 3 years thereafter.[13][14][19]
Guidelines differ with regard to the size threshold at which asymptomatic polyps of the small bowel should be removed, although all concur that any symptomatic polyps should be excised regardless of size. US guidelines recommend removal of asymptomatic polyps ≥10 millimetres in diameter, whereas European guidelines recommend a higher threshold of >15-20 millimetres.[13][14][19][20][22][33]
Polypectomy is achieved via upper endoscopy or single or double balloon enteroscopy depending on the location of polyps. One series of 34 patients with small bowel hamartomatous polyposis found that double balloon enteroscopy was successful in more than 80% of patients and had an acceptable margin of safety.[39] Surgery may be required in the presence of neoplasia, or if polyp size or number preclude endoscopic removal. It may also be required in patients with intussusception or small bowel obstruction. Some authorities recommend an attempt to clear the small intestine of polyps during laparotomy by means of intraoperative endoscopy with polypectomy or, for larger polyps, by means of enterotomy. This aggressive approach to the diagnosis and resection of small bowel polyps ('clean sweep') has been associated with a longer interval between subsequent surgeries and a decrease in total operations.[14][35][36][37]
There are limited data to advise on the size of polyps which merit polypectomy in the stomach or colon.[13] The US Multi-Society Task Force on Colorectal Cancer is the only organisation to provide a specific recommendation, advising removal of polyps >5 millimetres in diameter and an attempt to remove all polyps if endoscopically feasible.[14] Colectomy is sometimes necessary and should be considered if colonoscopic management is difficult and especially if neoplastic change is found in colonic polyps.[4][Figure caption and citation for the preceding image starts]: Small bowel hamartomatous polyp identified on capsule endoscopyFrom the collection of Dr Carol A. Burke, used with permission [Citation ends].
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer