Cancer surveillance screening for patients with PJS
Cancer screening and surveillance is indicated in all individuals with PJS.
Limited data exist regarding the efficacy of the various cancer surveillance modalities for patients with PJS. Guidelines for cancer screening are largely based on expert opinion.
Gastrointestinal cancer
US and European guidelines, along with consensus statements, make the following recommendations regarding gastrointestinal surveillance:[13]Latchford A, Cohen S, Auth M, et al. Management of Peutz-Jeghers syndrome in children and adolescents: a position paper from the ESPGHAN Polyposis Working Group. J Pediatr Gastroenterol Nutr. 2019 Mar;68(3):442-52.
https://journals.lww.com/jpgn/Fulltext/2019/03000/Management_of_Peutz_Jeghers_Syndrome_in_Children.31.aspx
http://www.ncbi.nlm.nih.gov/pubmed/30585892?tool=bestpractice.com
[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
[19]Monahan KJ, Bradshaw N, Dolwani S, et al. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut. 2020 Mar;69(3):411-44.
https://gut.bmj.com/content/69/3/411.long
http://www.ncbi.nlm.nih.gov/pubmed/31780574?tool=bestpractice.com
[20]van Leerdam ME, Roos VH, van Hooft JE, et al. Endoscopic management of polyposis syndromes: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2019 Sep;51(9):877-95.
https://www.thieme-connect.com/products/ejournals/html/10.1055/a-0965-0605
http://www.ncbi.nlm.nih.gov/pubmed/31342472?tool=bestpractice.com
[22]Wagner A, Aretz S, Auranen A, et al. The management of Peutz-Jeghers syndrome: European Hereditary Tumour Group (EHTG) guideline. J Clin Med. 2021 Jan 27;10(3):473.
https://www.mdpi.com/2077-0383/10/3/473/htm
http://www.ncbi.nlm.nih.gov/pubmed/33513864?tool=bestpractice.com
[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
Video capsule endoscopy (VCE) or magnetic resonance enterography (MRE) of the small bowel should begin by age 8 years (or earlier if the patient is symptomatic). Capsule endoscopy is safe to use in individuals with PJS and small bowel polyposis who do not have obstructive symptoms. If a concern for capsule retention is present, a patency capsule should be utilised. If no polyps are found at the initial examination, US guidelines recommend that small bowel surveillance should resume at age 18 years and continue every 2-3 years throughout life, whereas European guidelines advise repeating surveillance every 3 years from the outset.[13]Latchford A, Cohen S, Auth M, et al. Management of Peutz-Jeghers syndrome in children and adolescents: a position paper from the ESPGHAN Polyposis Working Group. J Pediatr Gastroenterol Nutr. 2019 Mar;68(3):442-52.
https://journals.lww.com/jpgn/Fulltext/2019/03000/Management_of_Peutz_Jeghers_Syndrome_in_Children.31.aspx
http://www.ncbi.nlm.nih.gov/pubmed/30585892?tool=bestpractice.com
[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
[19]Monahan KJ, Bradshaw N, Dolwani S, et al. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut. 2020 Mar;69(3):411-44.
https://gut.bmj.com/content/69/3/411.long
http://www.ncbi.nlm.nih.gov/pubmed/31780574?tool=bestpractice.com
[20]van Leerdam ME, Roos VH, van Hooft JE, et al. Endoscopic management of polyposis syndromes: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2019 Sep;51(9):877-95.
https://www.thieme-connect.com/products/ejournals/html/10.1055/a-0965-0605
http://www.ncbi.nlm.nih.gov/pubmed/31342472?tool=bestpractice.com
[22]Wagner A, Aretz S, Auranen A, et al. The management of Peutz-Jeghers syndrome: European Hereditary Tumour Group (EHTG) guideline. J Clin Med. 2021 Jan 27;10(3):473.
https://www.mdpi.com/2077-0383/10/3/473/htm
http://www.ncbi.nlm.nih.gov/pubmed/33513864?tool=bestpractice.com
[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
Oesophagogastroduodenoscopy (OGD) and colonoscopy to look for upper gastrointestinal and colorectal polyps should be done by age 8 years. If polyps are found, both examinations are repeated every 3 years; if no polyps are detected, a subsequent baseline examination is conducted at age 18 years, and every 3 years thereafter.[13]Latchford A, Cohen S, Auth M, et al. Management of Peutz-Jeghers syndrome in children and adolescents: a position paper from the ESPGHAN Polyposis Working Group. J Pediatr Gastroenterol Nutr. 2019 Mar;68(3):442-52.
https://journals.lww.com/jpgn/Fulltext/2019/03000/Management_of_Peutz_Jeghers_Syndrome_in_Children.31.aspx
http://www.ncbi.nlm.nih.gov/pubmed/30585892?tool=bestpractice.com
[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
[19]Monahan KJ, Bradshaw N, Dolwani S, et al. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut. 2020 Mar;69(3):411-44.
https://gut.bmj.com/content/69/3/411.long
http://www.ncbi.nlm.nih.gov/pubmed/31780574?tool=bestpractice.com
Breast cancer
The risk of breast cancer in women with PJS is similar to carriers of BRCA1 or BRCA2 mutations (40% to 85% lifetime risk).[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
The US Multi-Society Task Force on Colorectal Cancer advises monthly breast self-examination starting at age 18 years, biannual clinical breast examination starting at age 25 years, annual breast magnetic resonance imaging (MRI) starting from age 25-29 years, and mammography with consideration of tomosynthesis (3-dimensional mammography) alternating every 6 months with breast MRI with contrast from age 30-75 years.[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
The National Comprehensive Cancer Network (NCCN) recommends mammogram and MRI annually along with a clinical breast examination every 6 months, starting at approximately age 30 years.[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
Prophylactic mastectomy can be considered on a case-by-case basis.[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
Pancreatic cancer
Pancreatic cancer is the third most common malignancy (after breast and colorectal) in people with PJS, with an 11% to 36% lifetime risk of pancreatic ductal adenocarcinoma.[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
Surveillance via endoscopic ultrasound (EUS) and/or MRI or magnetic resonance cholangiopancreatography (MRCP) is recommended. The International Cancer of the Pancreas Screening Consortium recommends pancreatic imaging every 1-2 years starting from age 40 years.[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
[34]Canto MI, Harinck F, Hruban RH, et al. International Cancer of the Pancreas Screening (CAPS) Consortium summit on the management of patients with increased risk for familial pancreatic cancer. Gut. 2013 Mar;62(3):339-47.
https://gut.bmj.com/content/62/3/339.long
http://www.ncbi.nlm.nih.gov/pubmed/23135763?tool=bestpractice.com
The NCCN recommends annual imaging of the pancreas with either EUS or MRI/MRCP beginning at age 30-35 years.[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
Gynaecological cancers
The lifetime risks for ovarian, uterine, and cervical cancer are estimated at 21%, 9%, and 10% to 23%, respectively.[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
Guidelines differ with regard to the recommended age at which screening with pelvic examination, cervical smear, and transvaginal ultrasound should start, with the NCCN advising a starting age of approximately 18-20 years and other societies a later starting age of 25 years.[4]Syngal S, Brand RE, Church JM, et al; American College of Gastroenterology. ACG clinical guideline: genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015 Feb;110(2):223-62.
https://journals.lww.com/ajg/Fulltext/2015/02000/ACG_Clinical_Guideline__Genetic_Testing_and.8.aspx
http://www.ncbi.nlm.nih.gov/pubmed/25645574?tool=bestpractice.com
[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
Almost all ovarian cancers in patients with PJS are sex cord tumours with annular tubules (SCTAT). These tumours can cause irregular menstruation and precocious puberty. Annual physical examination to check for precocious puberty is recommended, starting at age 8 years, as well as yearly pelvic examination and pelvic ultrasound from the age of 18-25 years.[4]Syngal S, Brand RE, Church JM, et al; American College of Gastroenterology. ACG clinical guideline: genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015 Feb;110(2):223-62.
https://journals.lww.com/ajg/Fulltext/2015/02000/ACG_Clinical_Guideline__Genetic_Testing_and.8.aspx
http://www.ncbi.nlm.nih.gov/pubmed/25645574?tool=bestpractice.com
[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
For uterine cancer surveillance, annual pelvic examination is recommended from age 18-25 years. The American College of Gastroenterology (ACG) advises annual transvaginal ultrasound beginning at age 25 years.[4]Syngal S, Brand RE, Church JM, et al; American College of Gastroenterology. ACG clinical guideline: genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015 Feb;110(2):223-62.
https://journals.lww.com/ajg/Fulltext/2015/02000/ACG_Clinical_Guideline__Genetic_Testing_and.8.aspx
http://www.ncbi.nlm.nih.gov/pubmed/25645574?tool=bestpractice.com
The NCCN does not recommend routine ultrasound screening, but advises endometrial biopsy in the presence of abnormal bleeding.[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
A high proportion of cervical cancers in patients with PJS are minimal deviation adenocarcinoma (formerly known as adenoma malignum), a rare, well-differentiated adenocarcinoma that is difficult to detect with liquid-based cytology and has a poor prognosis. Guidelines recommend annual pelvic examination and liquid-based cytology from the age of 18-25 years (again, guidelines differ with regard to the age at which this should start).[4]Syngal S, Brand RE, Church JM, et al; American College of Gastroenterology. ACG clinical guideline: genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015 Feb;110(2):223-62.
https://journals.lww.com/ajg/Fulltext/2015/02000/ACG_Clinical_Guideline__Genetic_Testing_and.8.aspx
http://www.ncbi.nlm.nih.gov/pubmed/25645574?tool=bestpractice.com
[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
The NCCN also advocates consideration of total hysterectomy once a woman has completed her family.[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
Testicular cancer
Male patients with PJS have a 9% lifetime risk of developing Sertoli cell tumours, with a mean age at diagnosis of 9 years.[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
Annual testicular examination and observation for feminising changes is recommended, with follow-up testicular ultrasound if abnormalities are detected. The age at which this should start is controversial; the US Multi-Society Task Force on Colorectal Cancer advises screening from birth, whereas the NCCN recommends a higher starting age of approximately 10 years.[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
Lung cancer
The estimated lifetime risk of lung cancer in patients with PJS is 7% to 17%.[4]Syngal S, Brand RE, Church JM, et al; American College of Gastroenterology. ACG clinical guideline: genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015 Feb;110(2):223-62.
https://journals.lww.com/ajg/Fulltext/2015/02000/ACG_Clinical_Guideline__Genetic_Testing_and.8.aspx
http://www.ncbi.nlm.nih.gov/pubmed/25645574?tool=bestpractice.com
Guidelines differ in recommendations for surveillance. The US Multi-Society Task Force on Colorectal Cancer and NCCN simply recommend educating patients about symptoms and smoking cessation.[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
[33]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: genetic/familial high-risk assessment: colorectal [internet publication].
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436
However, the American College of Chest Physicians, American Society of Clinical Oncology, and American Cancer Society advise low-dose computed tomography (CT) annually from age 55-74 years (based on the level of cumulative risk in patients with PJS, which is similar to people with a more than 30 pack-year history of smoking who have quit for 10-15 years).[14]Boland CR, Idos GE, Durno C, et al. Diagnosis and management of cancer risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022 Jun;162(7):2063-85.
https://www.gastrojournal.org/article/S0016-5085(22)00151-2/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/35487791?tool=bestpractice.com
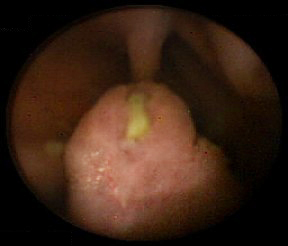
The evidence to support these recommendations is not robust. It is the opinion of the authors that surveillance should be individualised based on phenotype, expected age and incidence of disease, and family history. [Figure caption and citation for the preceding image starts]: Small bowel hamartomatous polyp identified on capsule endoscopyFrom the collection of Dr Carol A. Burke, used with permission [Citation ends].