History and exam
Key diagnostic factors
common
presence of risk factors
Key risk factors include lighter skin type and exposure to triggers such as hot baths/showers, temperature extremes, sunlight, alcohol, and emotional stress.
flushing
An early and sometimes diagnostic feature. However, not all people with rosacea report flushing, and those that do report flushing as their only symptom do not always develop the condition.[38]
erythema
Some level of erythema is seen in virtually all people with rosacea early in the course of the disorder. All people with the condition present with or describe some degree of redness. In patients with Fitzpatrick skin type V or VI (skin that rarely or never burns), erythema may be difficult to detect.
As the condition progresses, transient erythema may become persistent.[Figure caption and citation for the preceding image starts]: Rosacea with erythema, papules, and pustulesCourtesy of Dr Richard Allen Johnson (MD, CM. Harvard Medical School); used with permission [Citation ends].
papules and pustules
Present in progressive disease. May be the first clearly visible signs of rosacea in people with Fitzpatrick skin type V or VI (skin that rarely or never burns).
telangiectases
Superficial capillaries are one of the hallmarks of the disease, although their presence is not necessary for the diagnosis. Often, they are the most bothersome feature for people with the condition. Predominantly centrofacial in people with Fitzpatrick skin types I to IV. In people with skin types V or VI, a dermatoscope may aid detection of telangiectases.
ocular manifestations
People with rosacea typically describe a foreign body sensation in the eye, often with tearing, pain, and blurry vision.
There are often telangiectases and erythema of the lid margin, sometimes with scaling.
Other ocular manifestations include recurrent chalazion or hordeolum, keratitis, episcleritis, and scleritis.[1][38]
It is not uncommon for people to present with signs and symptoms suggestive of conjunctivitis and blepharitis, and for these to be significant manifestations of rosacea.
Ocular findings are the initial presentation in up to 20% of patients, some of whom may never progress to other phenotypes.[16][Figure caption and citation for the preceding image starts]: Ocular rosacea presenting as chalazionCourtesy of Dr Richard Allen Johnson (MD, CM. Harvard Medical School); used with permission [Citation ends].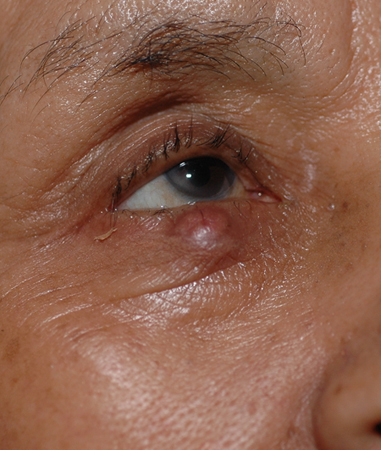
plaque formation
Severe papulopustular rosacea can evolve with coalescent lesions forming erythematous or violaceous plaques.
facial distribution
Rosacea primarily affects the convexities of the central face, including the cheeks, chin, nose, and central forehead.[1]
uncommon
phymatous changes
The most frequent is rhinophyma (commonly known as 'whiskey nose' or 'rum blossom').
This severe form of sebaceous gland hyperplasia is 20 times more common in men than women.
Rhinophyma is often referred to as end-stage rosacea, but it can be seen even when other features of the disease are mild.[38][Figure caption and citation for the preceding image starts]: RhinophymaCourtesy of Dr Richard Allen Johnson (MD, CM. Harvard Medical School); used with permission [Citation ends].
Other diagnostic factors
common
acne vulgaris
May or may not co-exist.
uncommon
burning or stinging
Frequently described by people with erythema.
dry appearance
Skin may be rough and scaling.
oedema
Prominent papules and pustules give the appearance of swelling and can induce underlying oedema in the dermis.
This is an uncommon feature of progressive disease but is nonetheless considered a characteristic feature if present.
peripheral location
Flushing may involve the upper chest, neck, and back.
Risk factors
strong
Fitzpatrick skin type I or II
hot baths/showers
Cutaneous manifestations are exacerbated in predisposed people when exposed to hot baths or showers.[1]
temperature extremes
Extremes of temperature, particularly increased temperatures, are likely to elicit redness.[1]
sunlight
There is increased sun sensitivity in predisposed people. Direct sunlight has been clearly established as a trigger for exacerbation of cutaneous manifestations.[1]
emotional stress
The association between stress or anger and the development of signs is unclear. However, flushing is certainly elicited by both.[1]
hot drinks
This is one of the most notable triggers for flushing.[37]
family history
A cohort study of fraternal twins concluded that the genetic contribution to rosacea was 46%.[13]
female sex
In the UK, the overall incidence of diagnosed rosacea has been reported as 1.92 per 1000 person-years for women and 1.34 per 1000 person-years for men.[9] One meta-analysis of population-based studies from Europe, North America, Africa, Asia, and South America reported an estimated prevalence rate of 5.41% for women and 3.9% for men.[8] However, men with rosacea are more likely to progress to advanced disease.[6][8][9]
weak
spicy foods
Not all people experience a worsening of their condition when exposed to spicy foods; however, there appears to be an association.[1]
alcohol
Some of the skin findings, such as flushing, may be exacerbated when predisposed people consume alcohol. People with alcohol-use disorders are often thought to develop nose changes similar to those seen in phymatous rosacea; the role of alcohol in phymatous rosacea in particular is unclear.[1][Figure caption and citation for the preceding image starts]: RhinophymaCourtesy of Dr Richard Allen Johnson (MD, CM. Harvard Medical School); used with permission [Citation ends].
Use of this content is subject to our disclaimer