Tests
Tests to consider
ultrasound
Test
Initial imaging of superficial lesions, e.g., lesions on the extremities, head, or neck, is with ultrasound.[31][32] Ultrasound has a sensitivity of 87% and a specificity of 96% for diagnosis of lipoma.[33] Urgent investigation is recommended for an unexplained lump that is increasing in size, to evaluate for soft tissue sarcoma.[34]
Result
typically discrete, encapsulated, homogeneous mass
MRI
Test
MRI is requested if the initial ultrasound is nondiagnostic.[31] MRI can attenuate bone artifact and discern the relationship of the mass to fascial planes, vessels, bones, and nerves.[35][36][Figure caption and citation for the preceding image starts]: Intramuscular lipoma, right thigh. MRI, axial, T1-weighted image. Lipomatous mass in the anterior aspect of the right thighFrom the collection of Dr Kimberly Moore Dalal and Dr Steven D. DeMartini; used with permission [Citation ends].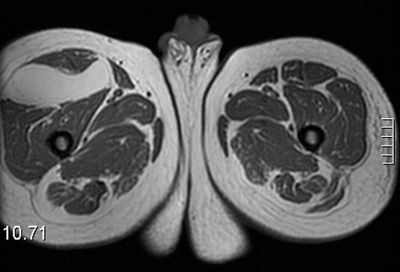 [Figure caption and citation for the preceding image starts]: Intramuscular lipoma, right thigh. MRI, coronal, T1-weighted image. Lipomatous mass in the anterior aspect of the right thighFrom the collection of Dr Kimberly Moore Dalal and Dr Steven D. DeMartini; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Intramuscular lipoma, right thigh. MRI, coronal, T1-weighted image. Lipomatous mass in the anterior aspect of the right thighFrom the collection of Dr Kimberly Moore Dalal and Dr Steven D. DeMartini; used with permission [Citation ends].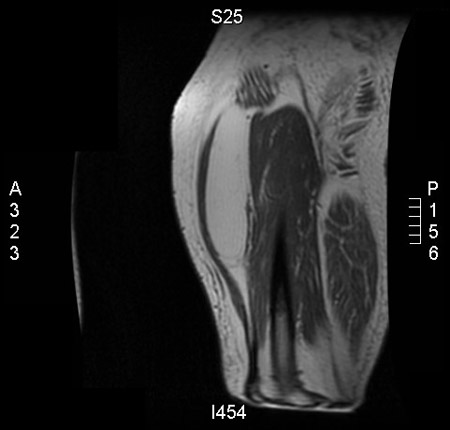
Result
typically discrete, encapsulated, homogeneous mass, with few or no thin, discrete septa and minimal or no areas of enhancement or high T2 signal
CT scan
Test
If a lesion is on the trunk, particularly if it seems deep to the superficial fascia, CT imaging is often preferred to MRI. CT with intravenous contrast may be ordered to evaluate deep tissue masses that are not amenable to ultrasound or radiographic evaluation.[31] In patients with large gastrointestinal lipomas, a CT scan will demonstrate Hounsfield units identical to fat.[29]
Result
typically discrete, encapsulated, homogeneous mass, with few or no thin, discrete septa; density similar to normal fat
core needle biopsy
Test
In an adult, any extremity or truncal soft-tissue mass that is symptomatic or enlarging, larger than 3 cm, or new and persisting beyond 4 weeks should be biopsied by core needle biopsy.
This provides accurate information for diagnosis and assessment of possible malignant potential and grade when read by an experienced pathologist.[39]
Should tissue be inadequate, a repeat core needle biopsy can be planned. If this is also nondiagnostic, an open linearly placed incisional biopsy along the longitudinal axis of the limb and wide excision of the mass can be performed.
Result
histologic appearance consistent with lipoma: subcutaneous lipomas are well-circumscribed, lobulated, mesenchymal tumors composed of adipocytes and demarcated from surrounding fat by a thin, fibrous capsule; angiolipomas are composed of adipocytes with interspersed clusters of capillaries containing fibrin thrombi; spindle cell lipomas are composed of collagen-forming spindle cells that have replaced mature fat; intramuscular lipomas are usually poorly circumscribed and infiltrative; and hibernomas resemble the glandular brown fat found in hibernating animals
incisional biopsy
Test
If repeat core needle biopsy is inconclusive, an incisional biopsy is indicated. Lesions on the limbs are best sampled through a longitudinal incision centered over the mass in its most superficial location. Wide excision of the mass is performed. A longitudinal incision is used so that the entire biopsy tract can be excised at the time of definitive resection and closed primarily.[16]
Result
histologic appearance consistent with lipoma: subcutaneous lipomas are well-circumscribed, lobulated, mesenchymal tumors composed of adipocytes and demarcated from surrounding fat by a thin, fibrous capsule; angiolipomas are composed of adipocytes with interspersed clusters of capillaries containing fibrin thrombi; spindle cell lipomas are composed of collagen-forming spindle cells that have replaced mature fat; intramuscular lipomas are usually poorly circumscribed and infiltrative; and hibernomas resemble the glandular brown fat found in hibernating animals
excisional biopsy
Test
Excisional biopsy is recommended for cutaneous or subcutaneous tumors more than 3 cm in size.[16]
Result
histologic appearance consistent with lipoma: subcutaneous lipomas are well-circumscribed, lobulated, mesenchymal tumors composed of adipocytes and demarcated from surrounding fat by a thin, fibrous capsule; angiolipomas are composed of adipocytes with interspersed clusters of capillaries containing fibrin thrombi; spindle cell lipomas are composed of collagen-forming spindle cells that have replaced mature fat; intramuscular lipomas are usually poorly circumscribed and infiltrative; and hibernomas resemble the glandular brown fat found in hibernating animals
upper gastrointestinal contrast study
gastrointestinal endoscopy
Test
Gastrointestinal lipomas that are encountered during upper endoscopy may be biopsied. Biopsy may not be required if the lipoma has typical clinical features.[29]
Result
lipomas have a typical yellowish appearance on white light endoscopy and demonstrate the "pillow sign" (the lipoma is easily deformed when pressed with closed biopsy forceps)
Use of this content is subject to our disclaimer